nodular ganglioneuroblastoma
Image Gallery
[ (||image_reduire{0,60}|inserer_attribut{alt,Nodular ganglioneuroblastoma}) ] [ (||image_reduire{0,60}|inserer_attribut{alt,Nodular ganglioneuroblastoma}) ]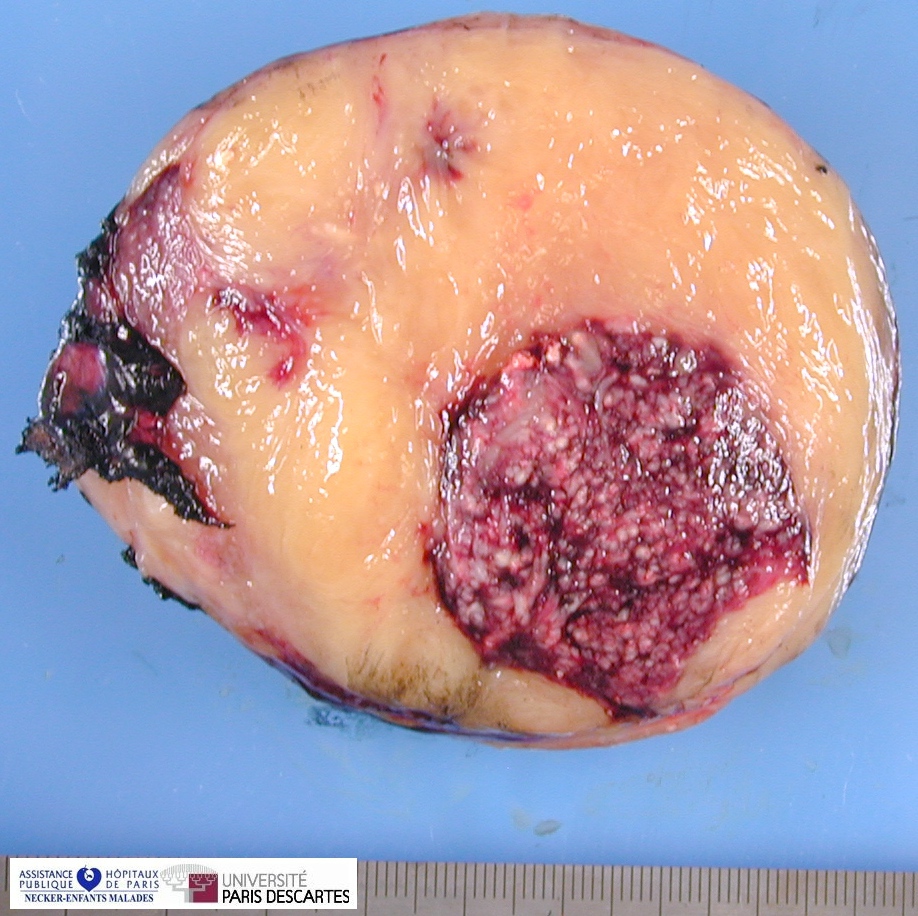{kind=link}
{kind=link}
Digital slides
![]() Case 26 : nodular ganglioneuroblastoma
Case 26 : nodular ganglioneuroblastoma
Definition: Ganglioneuroblastoma, nodular (GNBn) is a rare subtype of the family of neuroblastic tumors (neuroblastoma, ganglioneuroblastoma, and ganglioneuroma) that are classified in the unfavorable histology group according to the International Neuroblastoma Pathology Classification (INPC - Shimada system).
Tumors of this subtype have been considered to represent a prototypic example of biologically and clinically nonaggressive (Schwannian stroma-rich and stroma-dominant) components combined with biologically and clinically aggressive nodular (Schwannian stroma-poor) components. However, detailed histopathologic analysis as well as thorough prognostic evaluation of patients with this subtype has not been reported.
The nodular components in GNBn tumors are not always aggressive. The prognosis of these patients can be determined by the analysis of age-linked histopathologic features.
Patients with GNBn have a high potential for distant metastasis and have a poor clinical outcome.
Tumors in this subtype are comprised of different clones characterized by macroscopically visible and often hemorrhagic neuroblastomatous (Schwannian stroma-poor) nodule(s) coexisting with nonaggressive component(s) of either “ganglioneuroblastoma, intermixed (Schwannian stroma-rich)” or “ganglioneuroma (Schwannian stroma-dominant), maturing or mature” morphology.
Pathology
Nodular histology varied from tumor to tumor and even in the same tumor tissue.
In many tumors, a single nodular histology with the same grade of neuroblastic differentiation and the same MKI class was seen throughout a single nodule or multiple nodules in the same tumor tissues.
In some tumors, however, different nodular histologies were found in the different nodular lesions or even in a single nodular lesion from the same tumor.
The morphologic features used for evaluation of the nodular histology were the same as those used for the prognostic distinction of conventional neuroblastoma (stroma-poor) tumors, and included grade of neuroblastic differentiation (undifferentiated, poorly differentiated, or differentiating) and mitosis karyorrhexis-index (MKI) (low MKI, < 2% or < 100 per 5000 cells; intermediate MKI, 2-4% or 100-200 per 5000 cells; high MKI, of > 4% or > 200 per 5000 cells).
The favorable nodules (FNs) included:
![]() 1) poorly differentiated or differentiating neuroblastoma with a low or intermediate MKI diagnosed in patients younger than 1.5 years;
1) poorly differentiated or differentiating neuroblastoma with a low or intermediate MKI diagnosed in patients younger than 1.5 years;
![]() 2) differentiating neuroblastoma with a low MKI diagnosed in children ages 1.5-5.0 years.
2) differentiating neuroblastoma with a low MKI diagnosed in children ages 1.5-5.0 years.
The unfavorable nodules (UNs) included:
![]() 1) any neuroblastoma with a high MKI at any age,
1) any neuroblastoma with a high MKI at any age,
![]() 2) any neuroblastoma with an intermediate MKI in children older than 1.5 years,
2) any neuroblastoma with an intermediate MKI in children older than 1.5 years,
![]() 3) undifferentiated neuroblastoma at any age,
3) undifferentiated neuroblastoma at any age,
![]() 4) poorly differentiated neuroblastoma diagnosed in children older than 1.5 years,
4) poorly differentiated neuroblastoma diagnosed in children older than 1.5 years,
![]() 5) any neuroblastoma diagnosed in children age > 5.0 years.
5) any neuroblastoma diagnosed in children age > 5.0 years.
After nodular histology was determined, the GNBn tumors were classified into two prognostic subsets. The FS of GNBn included tumors that contained single or multiple favorable nodules (FNs). The US included tumors with single UNs or multiple nodules that contained at least one unfavorable nodule (UN).
![]() Classical GNB
Classical GNB
- Macroscopy: visible neuroblastomatous (usually hemorrhagic) nodule in a ganglioneuromatous component with features of ganglioneuroblastoma, intermixed or ganglioneuroma of maturing or mature subtype in the tumor outside the nodule;
- Microscopy: there is abrupt transition between the neuroblastomatous nodule and the surrounding ganglioneuromatous component with or without a capsule (rarely focal invasion of former into latter may be seen);
- the neuroblastomatous component usually is of the undifferentiated or poorly differentiated subtype and rarely is of the differentiating subtype
![]() Multiple nodules
Multiple nodules
- Macroscopically visible, two or more neuroblastomatous nodules with a ganglioneuromatous component in the remaining portion of the tumor;
- the features of the nodules are the same as in the classical form.
![]() Large nodules
Large nodules
- No macroscopically visible nodules on a ganglioneuromatous battleground;
- the tumor nodule(s) resembles neuroblastoma on macroscopic examination;
- however, on microscopic examination, a ganglioneuromatous component is found as a thin rim at the periphery of large neuroblastomatous mass or as the trabecular portion between multiple neuroblastomatous nodules
No nodule
- Primary tumor has features of ganglioneuroblastoma, intermixed or ganglioneuroma, but metastasis to lymph node, bone, or other site shows neuroblastomatous feature
History
In 1947, Stout first described a tumor containing fully malignant neuroblastomatous nodules coexisting with ganglioneuromatous tissue; he introduced the idea of a composite tumor for this subtype of NTs and suggested its aggressive clinical behavior.
Adam and Hochholzer, in 1981, also reported a poor prognosis for patients with this subtype of ganglioneuroblastoma. In 1984, Shimada et al. defined morphologic and clinical characteristics of this subtype, named it “stroma-rich (ganglioneuroblastoma), nodular,” and separated it from other subtypes of NTs.
In 1999, the International Neuroblastoma Pathology Committee (INPC) proposed a classification of NTs by adopting the original Shimada system. In their report, this subtype of NTs was renamed “ganglioneuroblastoma, nodular (composite, Schwannian stroma-rich/stroma-dominant and stroma-poor)” with a similar but more precisely defined morphologic description.
Although tumors of this subtype are classified into an unfavorable histology group by the Shimada system, the INPC suggested further histopathologic evaluation and analysis to more fully define the biologic and clinical characteristics of GNBns.
Subtypes
The GNBn subtype of neuroblastic disease, which is found rarely in infants and usually is diagnosed in older children age superior to 1 year, causes a significantly lower overall EFS rate for the patients than non-GNBn subtypes of NTs.
The literature suggests that this subtype represents a prototypic example of a composite tumor made up of biologically and clinically nonaggressive clone(s)—i.e., ganglioneuroblastoma, inter-mixed (Schwannian stroma-rich) or ganglioneuroma (Schwannian stroma-dominant) component(s)—and biologically and clinically aggressive clone(s)—i.e., neuroblastomatous (Schwannian stroma-poor) component(s).
The neuroblastomatous components in this subtype are not always aggressive and that the prognosis of patients can be determined by precise evaluation of histology.
The same age-linked criteria used for neuroblastoma (Schwannian stroma-poor) tumors are applicable to the nodular component for distinguishing FN and UN.
Two distinct prognostic subsets, FS and US, have been identified in the GNBn subtype.
Tumors in the FS are composed of :
![]() 1) a Schwannian stroma-rich/stroma-dominant component
1) a Schwannian stroma-rich/stroma-dominant component
![]() 2) the FN component.
2) the FN component.
These tumors are distributed evenly in all stages and show a significantly better EFS and survival rate than the US that are comparable to those of the FH group in non-GNBn subtypes.
Conversely, tumors in the US containing UN frequently present with distant metastasis and have a significantly lower EFS and survival rate that are comparable to those of the UH group in non-GNBn subtypes.
The FN component, although it is morphologically less mature than the stroma-rich/ stroma-dominant component in the same tumor tissue, may have the potential for differentiation and, thus, may belong in the age-matched maturational sequence of biologically favorable NTs defined by the Shimada system.
These FNs may proceed along their course of maturation and take on a stroma-rich/stroma-dominant histology, eventually losing the characteristic feature of macroscopically visible, nodular formation of composite tumors in older patients.
According to the Shimada system, histologic changes from stroma-poor to stroma-rich/stroma-dominant morphology of these FNs are expected to take place in patients before age 5 years.
By contrast, UN in the GNBn subtype would remain histopathologically unfavorable, regardless of patient age. This may be one of the reasons why more FS tumors than US tumors are diagnosed in younger children. It also may explain the fact that the vast majority of the tumors in older children that had a ganglioneuroma (Schwannian stroma-dominant) morphology did not have FN.
While handling surgically removed or biopsy samples of the NT, pathologists may encounter some difficulty in diagnosing this subtype of GNBn. Because it is a composite tumor comprised of different clones, careful examination and tissue sampling is critical for histologic as well as molecular evaluation.
Because the nodule(s) could be small in size, careful macroscopic examination and tissue sampling from any suspicious areas of the primary tumor tissue are required for diagnosing GNBn.
It should be added here that the very low incidence of MYCN-amplified tumors observed in this subtype may or may not have been the result of sampling error.
Pathologists also should be aware that the nodular histology of this subtype can vary from one nodule to another in the multiple nodular tumor, or even in the different microscopic fields of the same nodule of either single- or multiple-nodular tumors. Histologi-cally different nodules or areas in the same tumor need to be evaluated separately and individually for determination of UN or FN status. Those tumors that contain any UN component should be classified into the US.
The Schwannian stroma-rich/stroma-dominant component is classified into either “ganglioneuroblastoma, intermixed” or “ganglioneuroma, maturing or mature.”
For the nodular Schwannian stroma-poor component, the grade of neuroblastic differentiation and MKI need to be documented.
Next, the nodular histology (FN or UN) should be determined based on the Shimada system of age-linked histopathologic evaluation, so that each tumor can be classified as FS or US.
See also
![]() ganglioneuroblastomas
ganglioneuroblastomas
- intermixed ganglioneuroblastoma
![]() neuroblastic tumors
neuroblastic tumors
- neuroblastomas
References
![]() Histopathology Defines Prognostic Subsets of Ganglioneuroblastoma, Nodular. A Report from the Children’s Cancer Group (PDF)
Histopathology Defines Prognostic Subsets of Ganglioneuroblastoma, Nodular. A Report from the Children’s Cancer Group (PDF)
![]() Revision of the International Neuroblastoma Pathology Classification
Confirmation of favorable and unfavorable prognostic subsets in ganglioneuroblastoma, nodular. Cancer, Volume 98 Issue 10, Pages 2274 - 2281 (PDF)
Revision of the International Neuroblastoma Pathology Classification
Confirmation of favorable and unfavorable prognostic subsets in ganglioneuroblastoma, nodular. Cancer, Volume 98 Issue 10, Pages 2274 - 2281 (PDF)
![]() Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B. Terminology and morphologic criteria of neuroblastic tumors. Recommendations by the International Neuroblastoma Pathology Committee. Cancer . 1999; 86: 349-363.
Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B. Terminology and morphologic criteria of neuroblastic tumors. Recommendations by the International Neuroblastoma Pathology Committee. Cancer . 1999; 86: 349-363.
![]() Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B, et al. The International Neuroblastoma Pathology Classification (the Shimada System). Cancer . 1999; 86: 364-372.
Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B, et al. The International Neuroblastoma Pathology Classification (the Shimada System). Cancer . 1999; 86: 364-372.
![]() Joshi VV. Peripheral neuroblastic tumors: pathologic classification based on recommendations of International Neuroblastoma Pathology Committee (modification of Shimada classification). Pediatr Dev Pathol . 2000; 3: 184-189.
Joshi VV. Peripheral neuroblastic tumors: pathologic classification based on recommendations of International Neuroblastoma Pathology Committee (modification of Shimada classification). Pediatr Dev Pathol . 2000; 3: 184-189.
![]() Shimada H, Chatten J, Newton WA, et al. Histopathologic prognostic factors in neuroblastic tumors: definition of subtypes of ganglioneuroblastoma and age-linked classification of neuroblastomas. J Natl Cancer Inst . 1984; 73: 405-416.
Shimada H, Chatten J, Newton WA, et al. Histopathologic prognostic factors in neuroblastic tumors: definition of subtypes of ganglioneuroblastoma and age-linked classification of neuroblastomas. J Natl Cancer Inst . 1984; 73: 405-416.
![]() Joshi VV, Cantor AB, Altshuler G, et al. Recommendations for modification of terminology of neuroblastic tumors and prognostic significance of Shimada classification. Cancer . 1992; 69: 2183-2196.
Joshi VV, Cantor AB, Altshuler G, et al. Recommendations for modification of terminology of neuroblastic tumors and prognostic significance of Shimada classification. Cancer . 1992; 69: 2183-2196.
![]() Shimada H, Umehara S, Monobe Y, et al. International Neuroblastoma Pathology Classification for prognostic evaluation of patients with peripheral neuroblastic tumors: a report from the Children’s Cancer Group. Cancer . 2001; 92: 2451-2461.
Shimada H, Umehara S, Monobe Y, et al. International Neuroblastoma Pathology Classification for prognostic evaluation of patients with peripheral neuroblastic tumors: a report from the Children’s Cancer Group. Cancer . 2001; 92: 2451-2461.
![]() Umehara S, Nakagawa A, Matthay KK, et al. Histopathology defines prognostic subsets of ganglioneuroblastoma, nodular. Cancer . 2000; 89: 1150-1161.
Umehara S, Nakagawa A, Matthay KK, et al. Histopathology defines prognostic subsets of ganglioneuroblastoma, nodular. Cancer . 2000; 89: 1150-1161.
![]() Matthay KK, Perez C, Seeger RC, et al. Successful treatment of Stage III neuroblastoma based on prospective biologic staging: a Children’s Cancer Group Study. J Clin Oncol . 1998; 16: 1256-1264.
Matthay KK, Perez C, Seeger RC, et al. Successful treatment of Stage III neuroblastoma based on prospective biologic staging: a Children’s Cancer Group Study. J Clin Oncol . 1998; 16: 1256-1264.
![]() Matthay KK, Villablanca JG, Seeger RC, et al. Treatment of high-risk neuroblastoma with intensive chemotherapy, radiotherapy, autologous bone marrow transplantation, and 13-cis-retinoic acid. Children’s Cancer Group. N Engl J Med . 1999; 341: 1165-1173.
Matthay KK, Villablanca JG, Seeger RC, et al. Treatment of high-risk neuroblastoma with intensive chemotherapy, radiotherapy, autologous bone marrow transplantation, and 13-cis-retinoic acid. Children’s Cancer Group. N Engl J Med . 1999; 341: 1165-1173.
![]() Nickerson HJ, Matthay KK, Seeger RC, et al. Favorable biology and outcome of Stage IV-S neuroblastoma with supportive care or minimal therapy: a Children’s Cancer Group study. J Clin Oncol . 2000; 18: 477-486.
Nickerson HJ, Matthay KK, Seeger RC, et al. Favorable biology and outcome of Stage IV-S neuroblastoma with supportive care or minimal therapy: a Children’s Cancer Group study. J Clin Oncol . 2000; 18: 477-486.
![]() Perez CA, Matthay KK, Atkinson JB, et al. Biologic variables in the outcome of Stage I and II neuroblastoma treated with surgery as primary therapy: a Children’s Cancer Group study. J Clin Oncol . 2000; 18: 18-26.
Perez CA, Matthay KK, Atkinson JB, et al. Biologic variables in the outcome of Stage I and II neuroblastoma treated with surgery as primary therapy: a Children’s Cancer Group study. J Clin Oncol . 2000; 18: 18-26.
![]() Kaplan EL, Meier P. Nonparametric estimation from incomplete observation. J Am Stat Assoc . 1958; 53: 457-481.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observation. J Am Stat Assoc . 1958; 53: 457-481.
![]() Stout AP. Ganglioneuroma of the sympathetic nervous system. Surg Gynecol Obstet . 1947; 84: 101-110.
Stout AP. Ganglioneuroma of the sympathetic nervous system. Surg Gynecol Obstet . 1947; 84: 101-110.
![]() Joshi VV, Cantor AB, Altshuler G, et al. Conventional versus modified morphologic criteria for ganglioneuroblastoma. A review of cases from the Pediatric Oncology Group. Arch Pathol Lab Med . 1996; 120: 859-865.
Joshi VV, Cantor AB, Altshuler G, et al. Conventional versus modified morphologic criteria for ganglioneuroblastoma. A review of cases from the Pediatric Oncology Group. Arch Pathol Lab Med . 1996; 120: 859-865.
![]() Adam A, Hochholzer L. Ganglioneuroblastoma of the posterior mediastinum: a clinicopathologic review of 80 cases. Cancer . 1981; 47: 373-381.
Adam A, Hochholzer L. Ganglioneuroblastoma of the posterior mediastinum: a clinicopathologic review of 80 cases. Cancer . 1981; 47: 373-381.
![]() Schmidt ML, Salwen HR, Chagnovich D, Bauer KD, Crawford SE, Cohn SL. Evidence for molecular heterogeneity in human ganglioneuroblastoma. Pediatr Pathol . 1993; 13: 787-796.
Schmidt ML, Salwen HR, Chagnovich D, Bauer KD, Crawford SE, Cohn SL. Evidence for molecular heterogeneity in human ganglioneuroblastoma. Pediatr Pathol . 1993; 13: 787-796.