Home > G. Tumoral pathology > infantile hemangioma
infantile hemangioma
Thursday 11 March 2004
juvenile hemangioma, cellular hemangioma of infancy, common hemangioma of infancy; GLUT1+ infantile hemangioma
Digital Cases (Digital slides)
HPC/106 : GLUT1+ infantile hemangioma
HPC:186 : GLUT1+ infantile hemangioma
HPC:385 : GLUT1+ infantile hemangioma
Clinical synopsis
The typical infantile hemangioma appears postnataly, grows quickly, and regresses gradually in the first few years of life. Approximately one third of IH are present at birth.
Infantile hemangiomas progress through 3 stages: proliferative, involuting, and involuted. The proliferative phase is characterized by clinical growth. Once hemangiomas reach their maximum size, they begin to regress or involute. Histologically, this stage is characterized by endothelial apoptosis. Finally, the involuted stage of the hemangioma occurs when the original lesion is replaced by a connective tissue remnant. In contrast to hemangiomas, vascular malformations do not involute but continue to enlarge as the patient grows.
Morphological synopsis
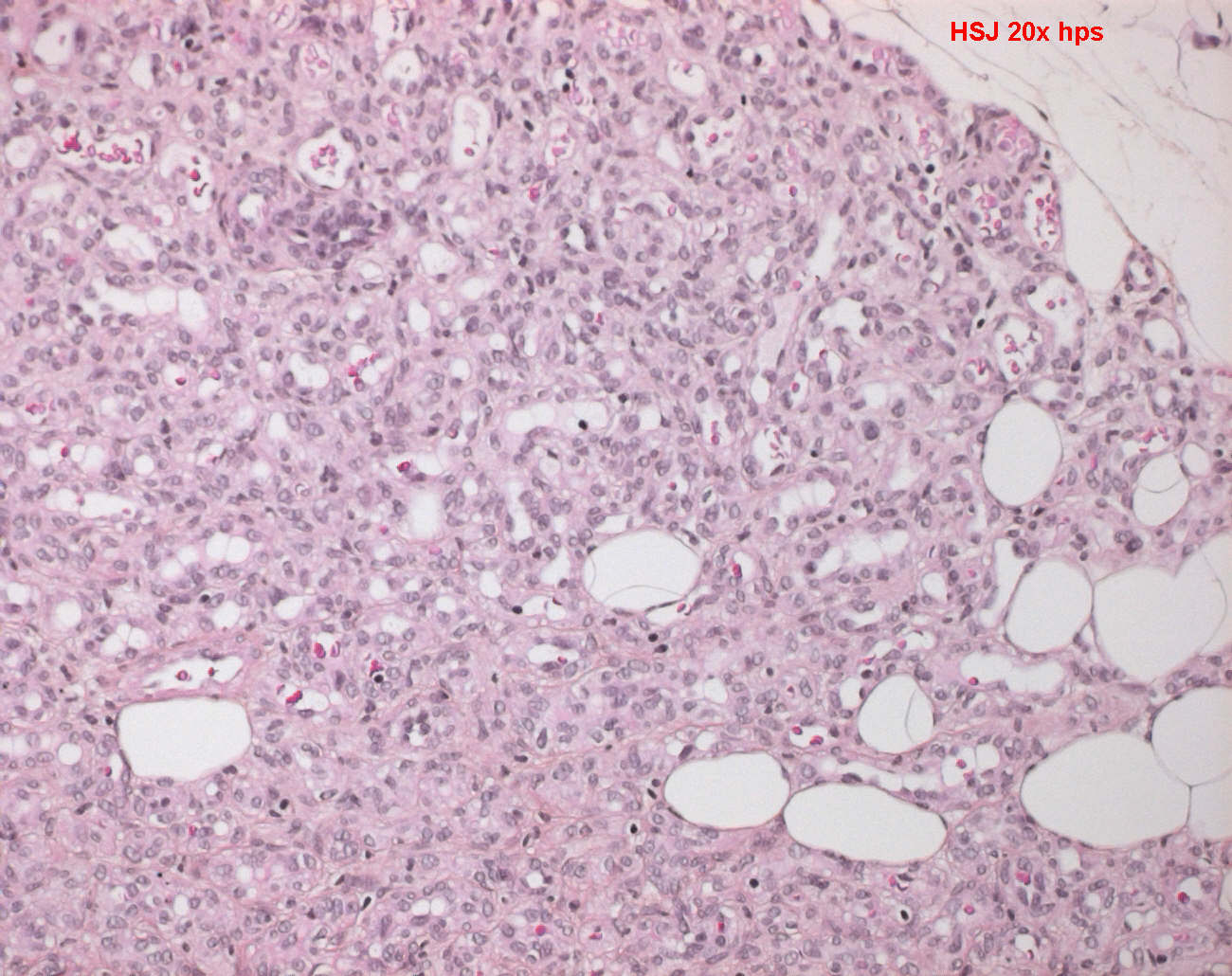
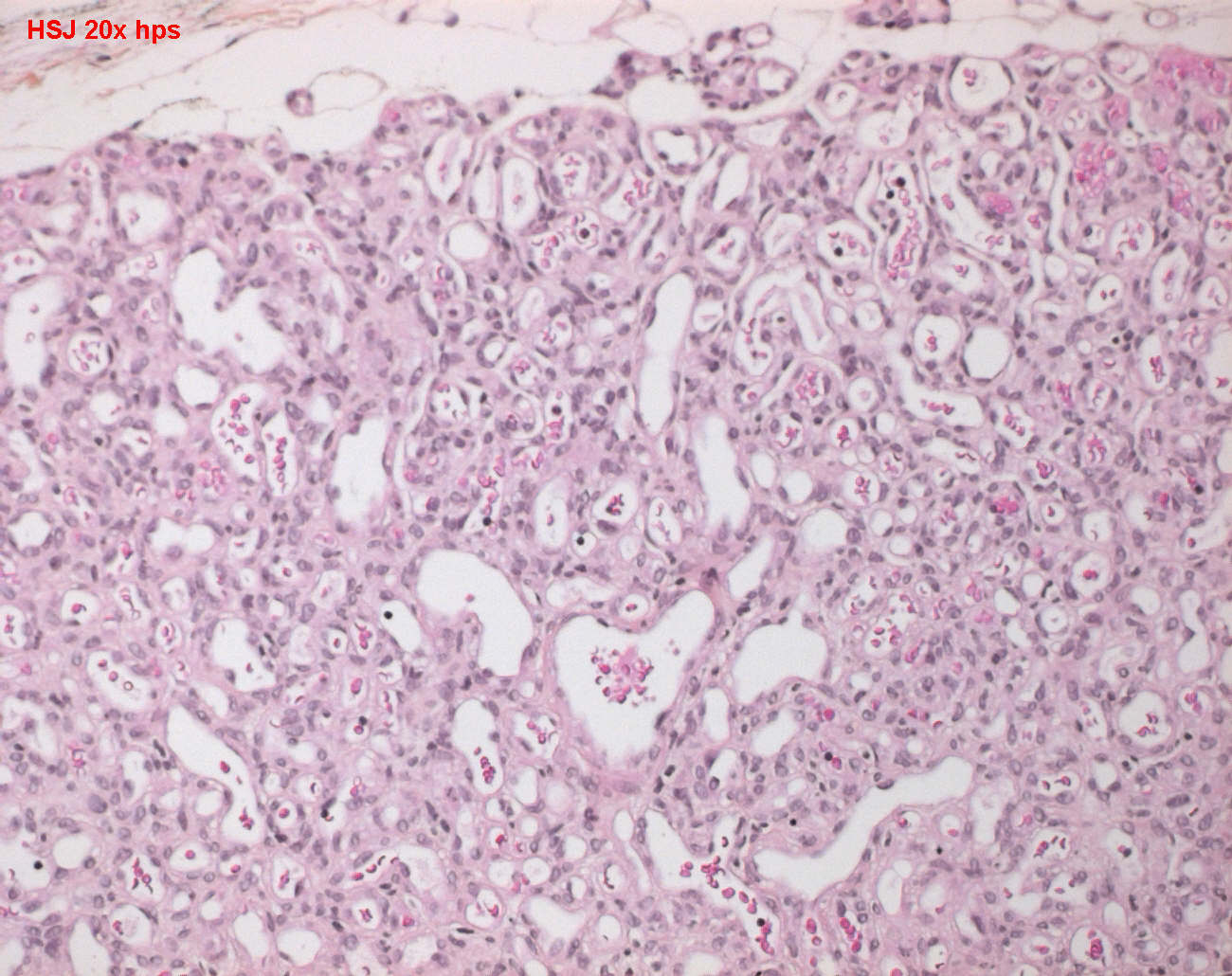
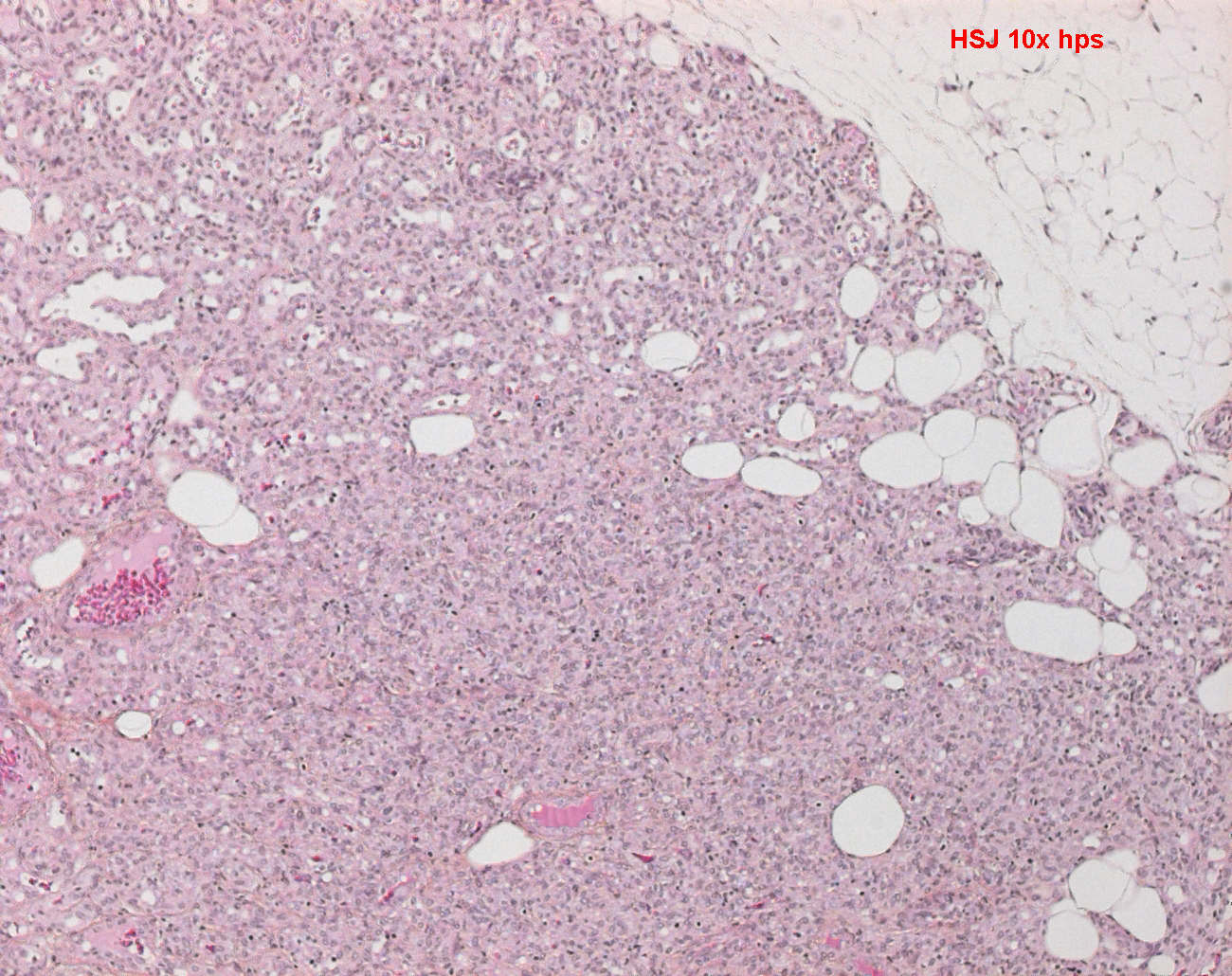
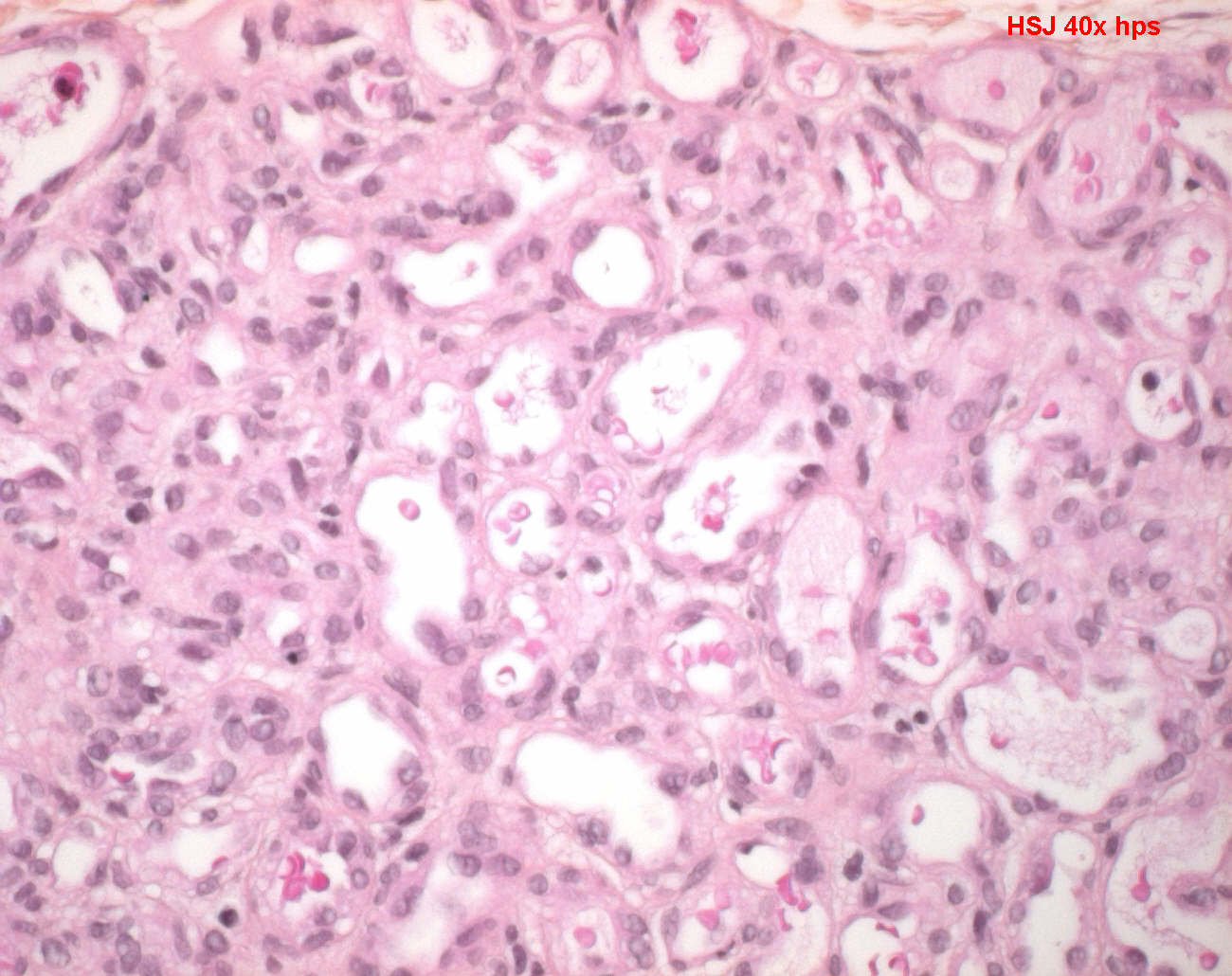
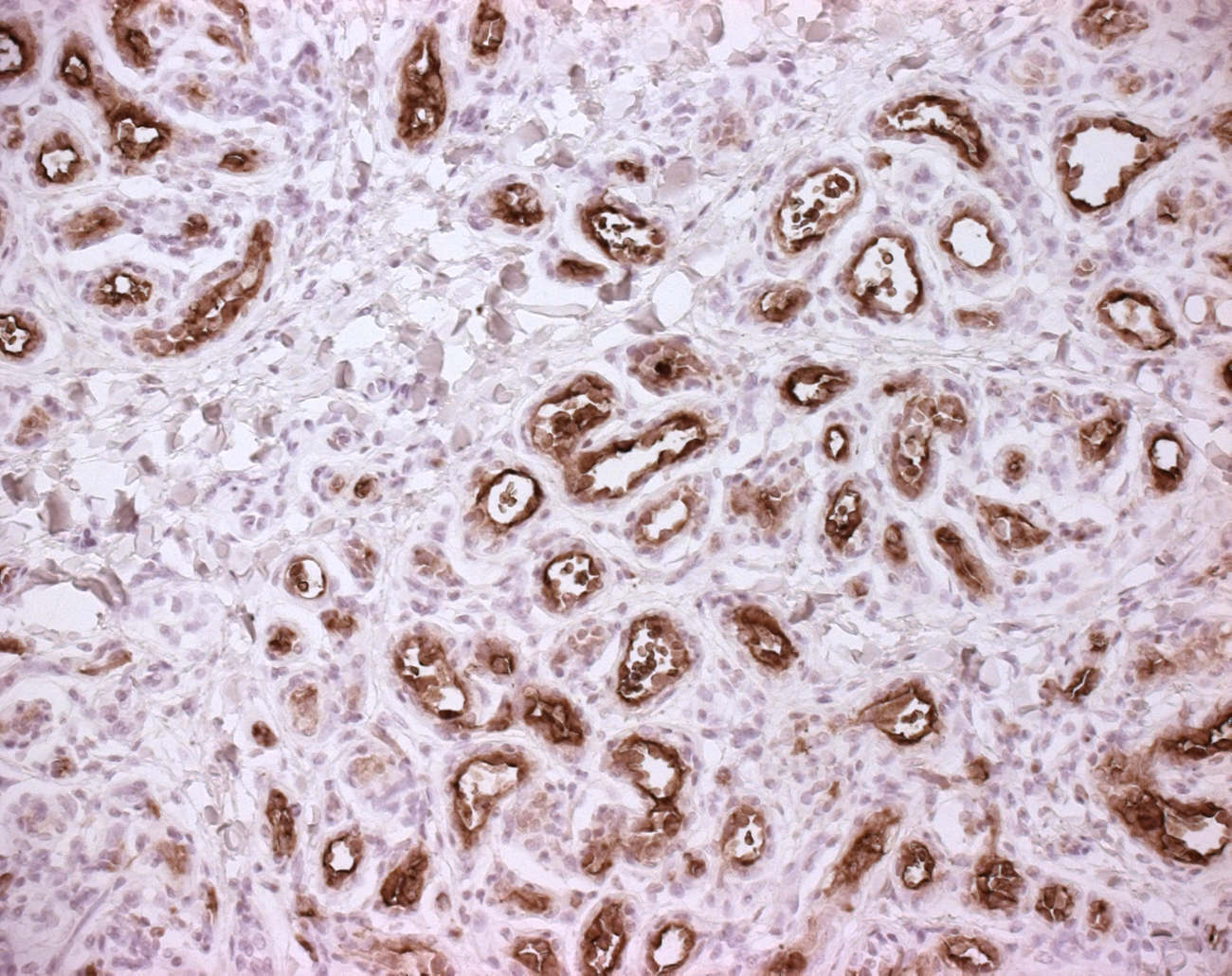
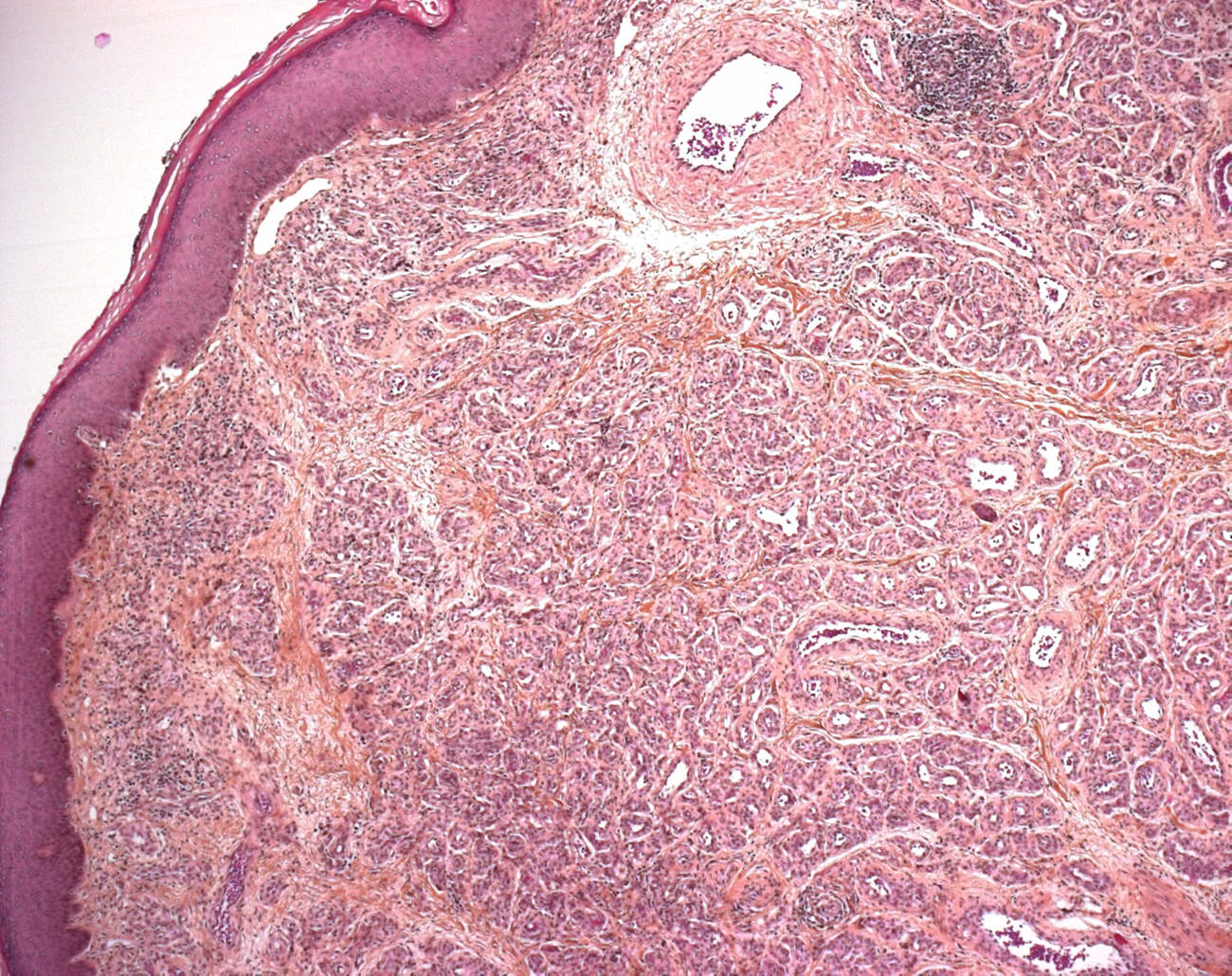
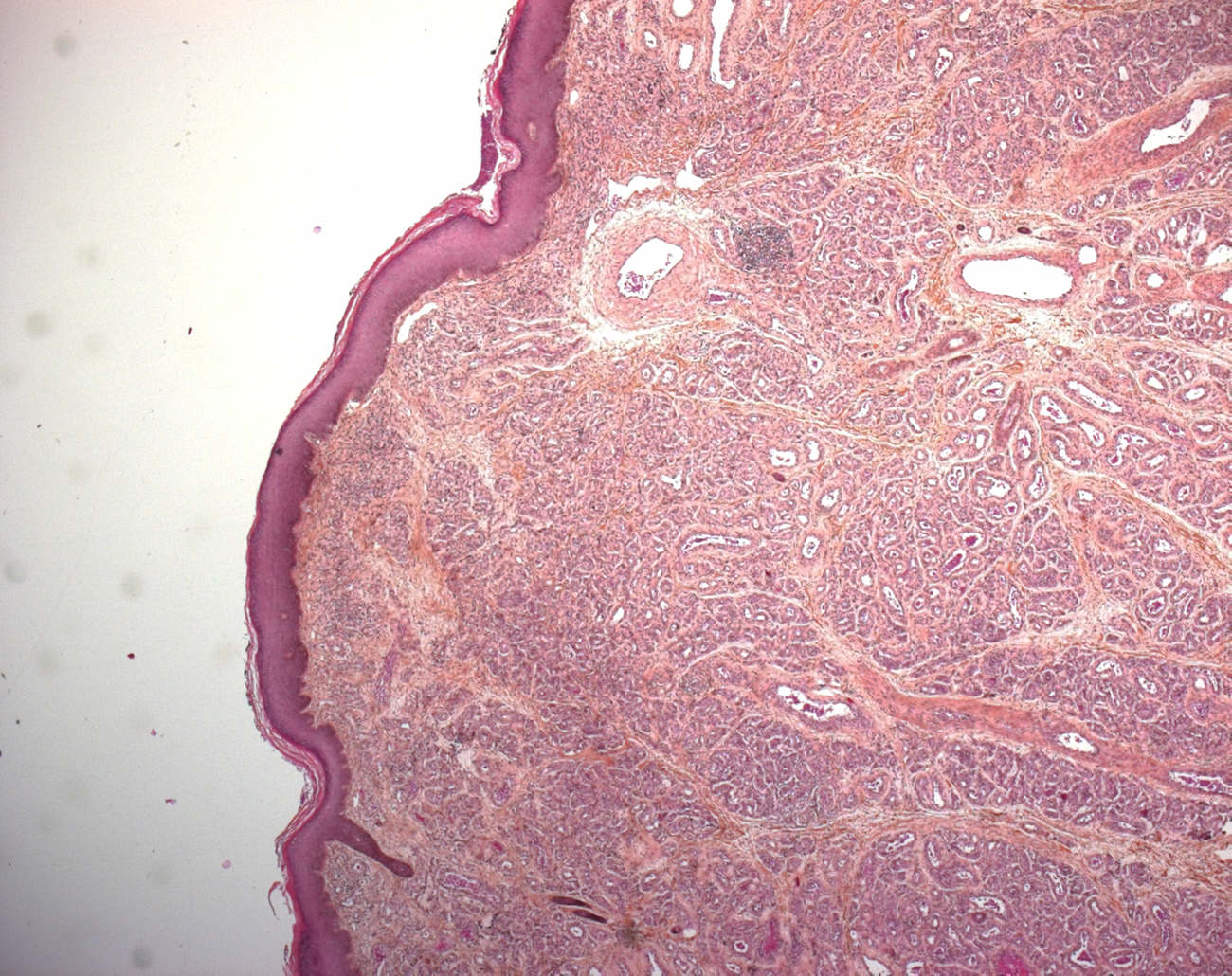
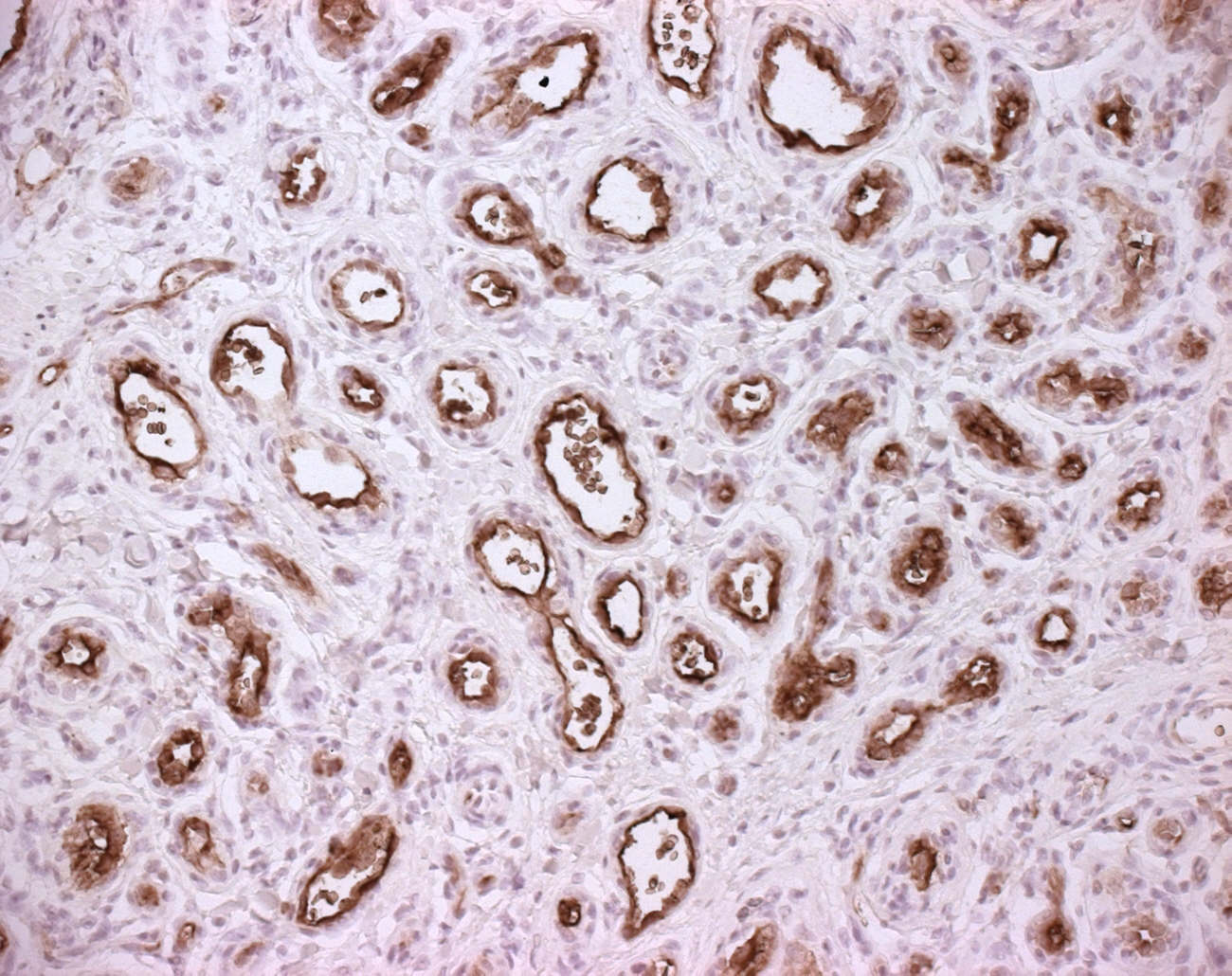
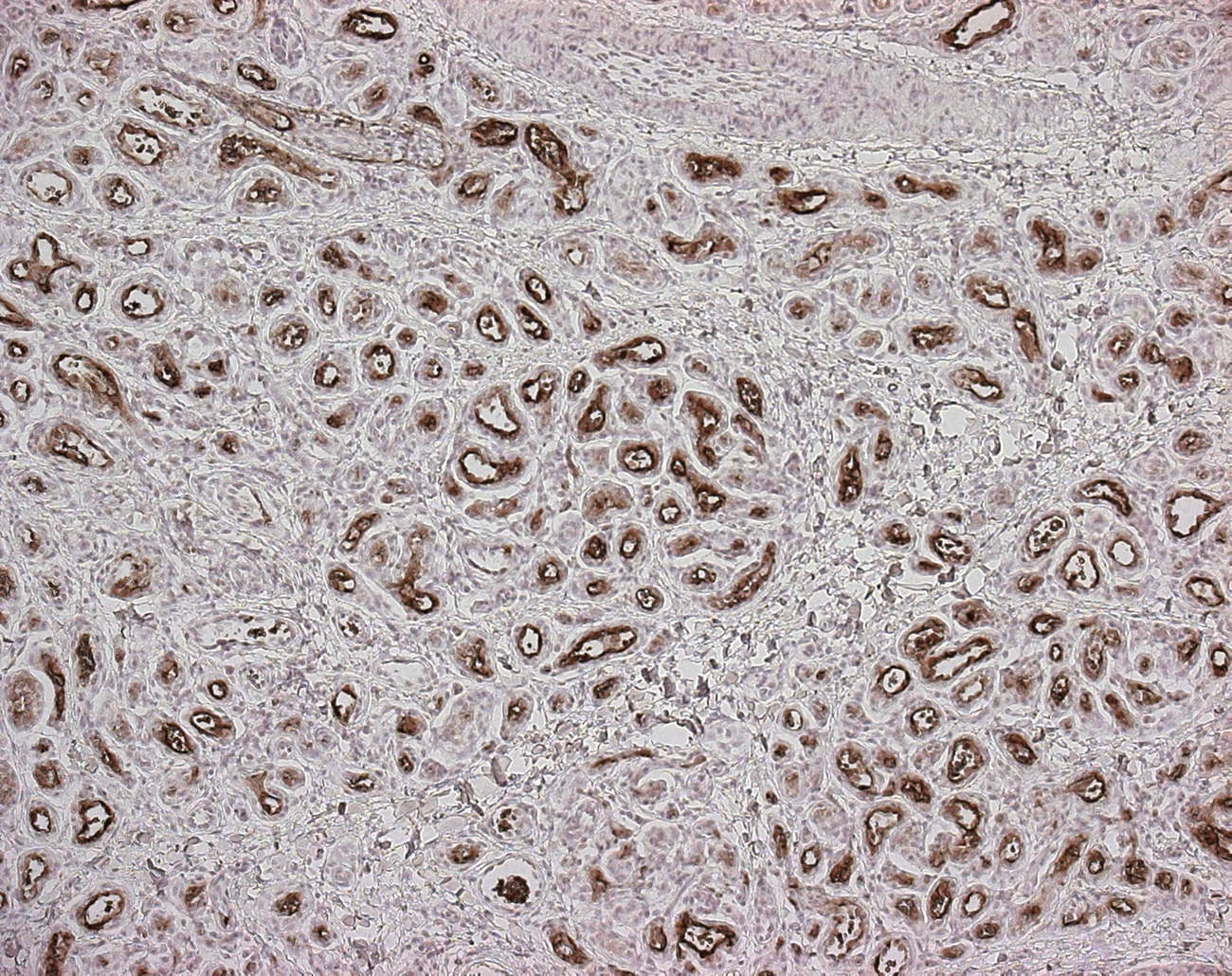
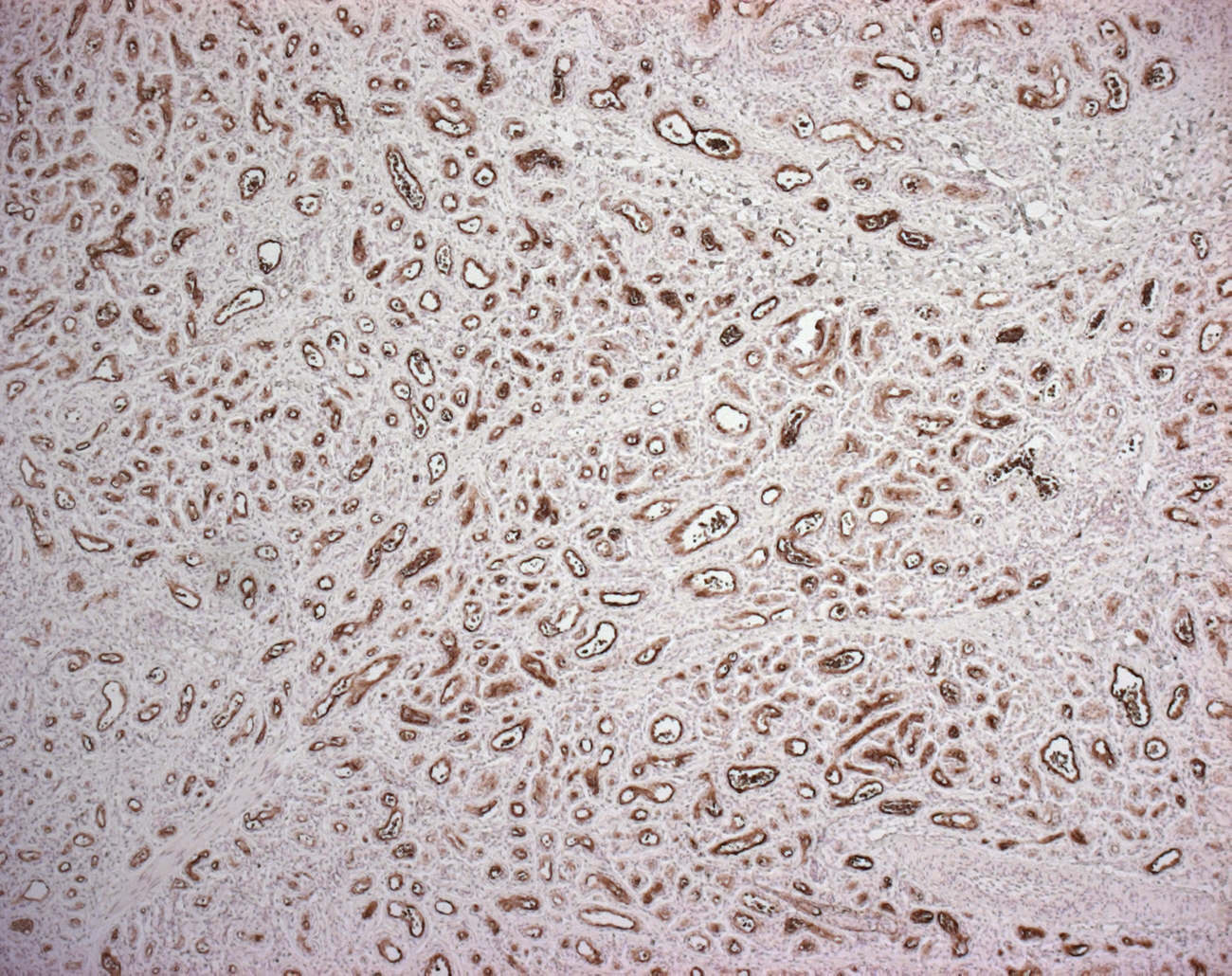
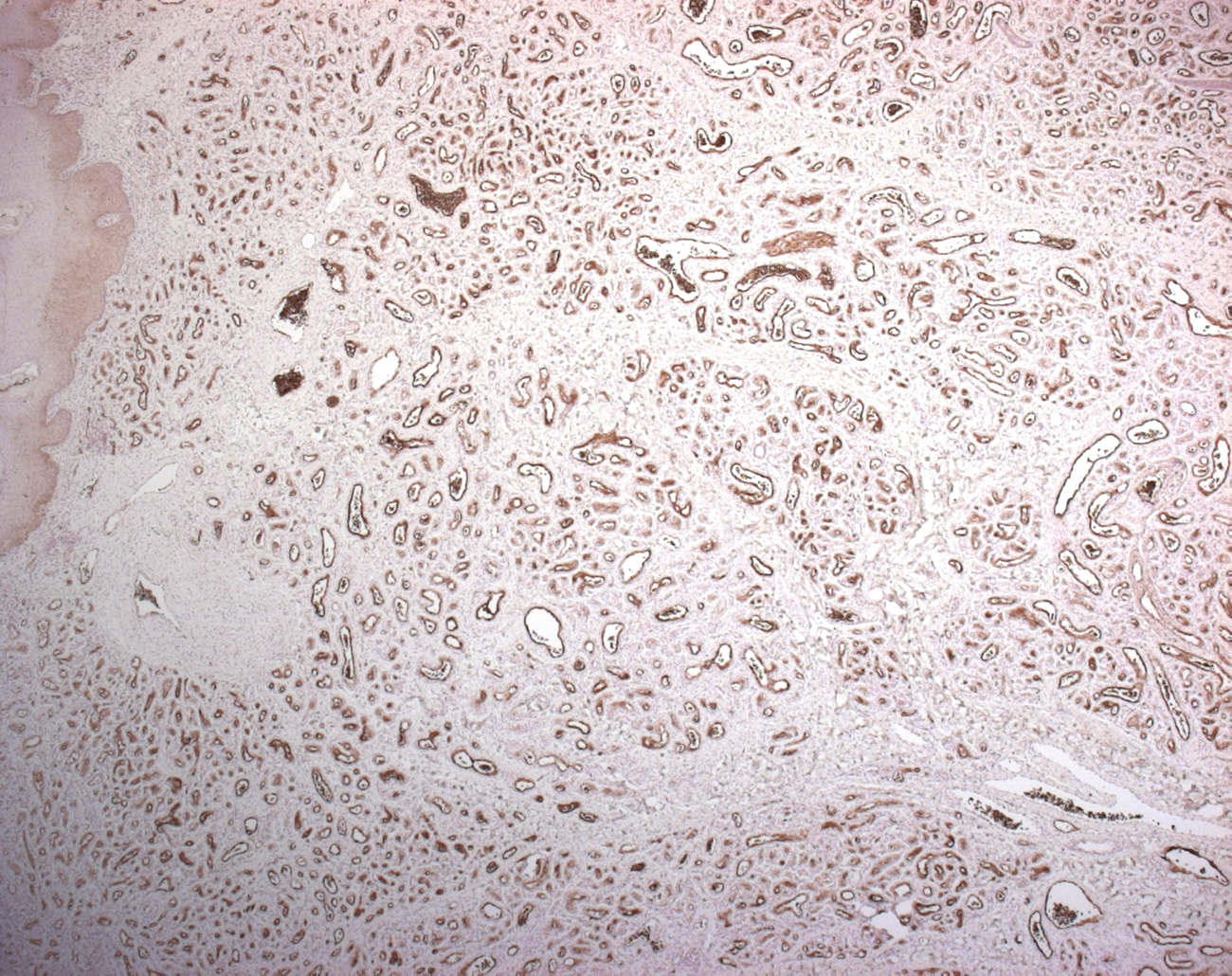
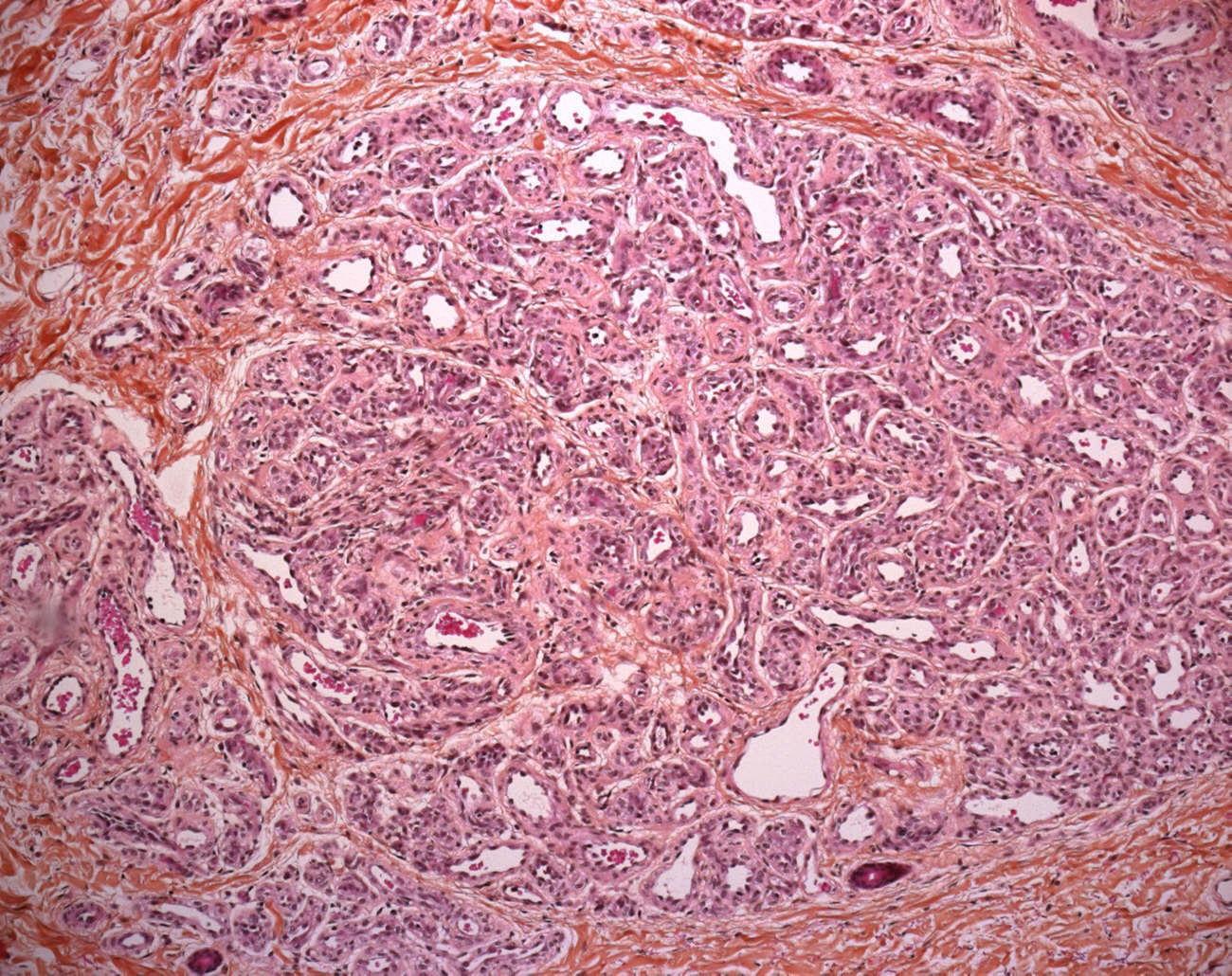
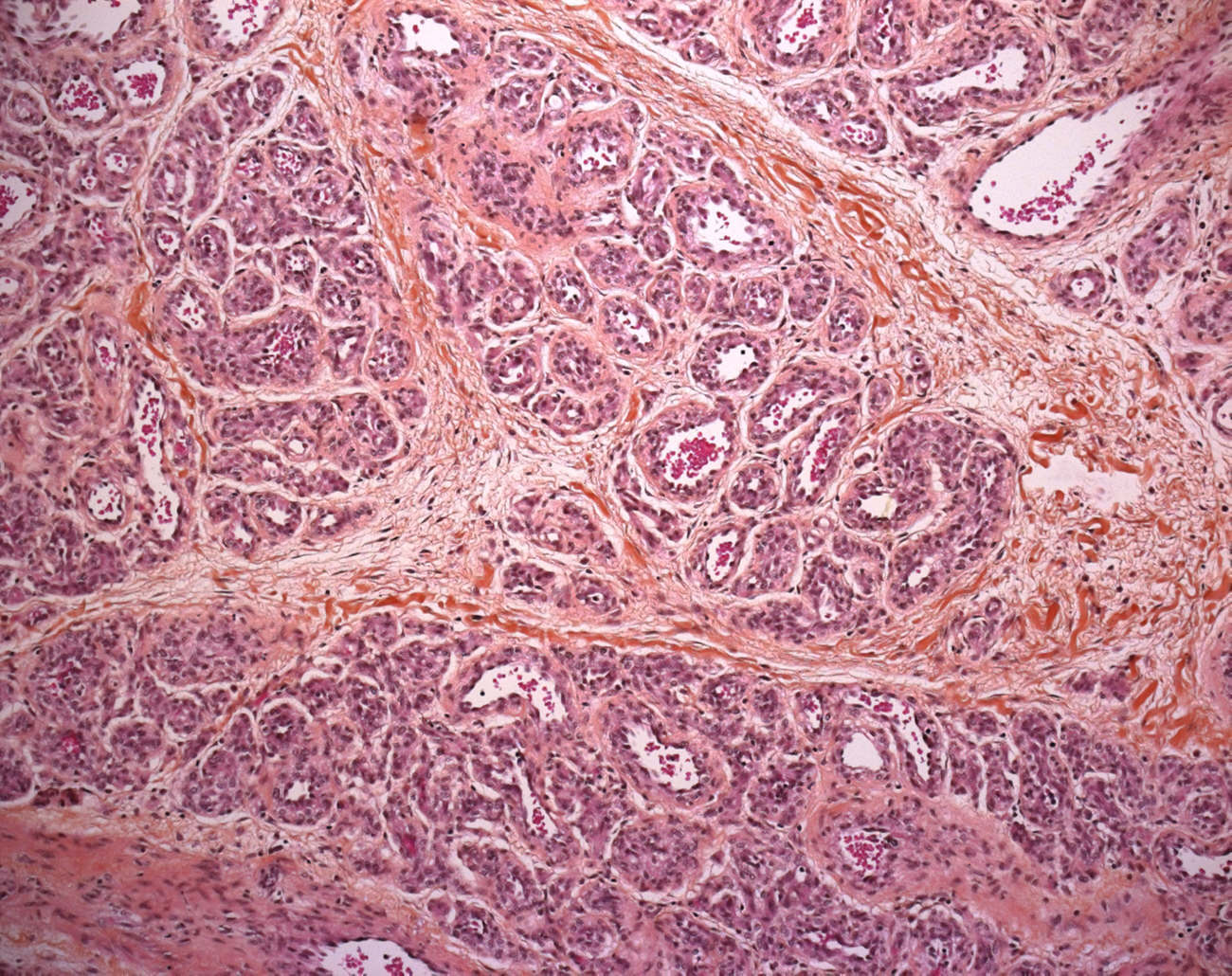
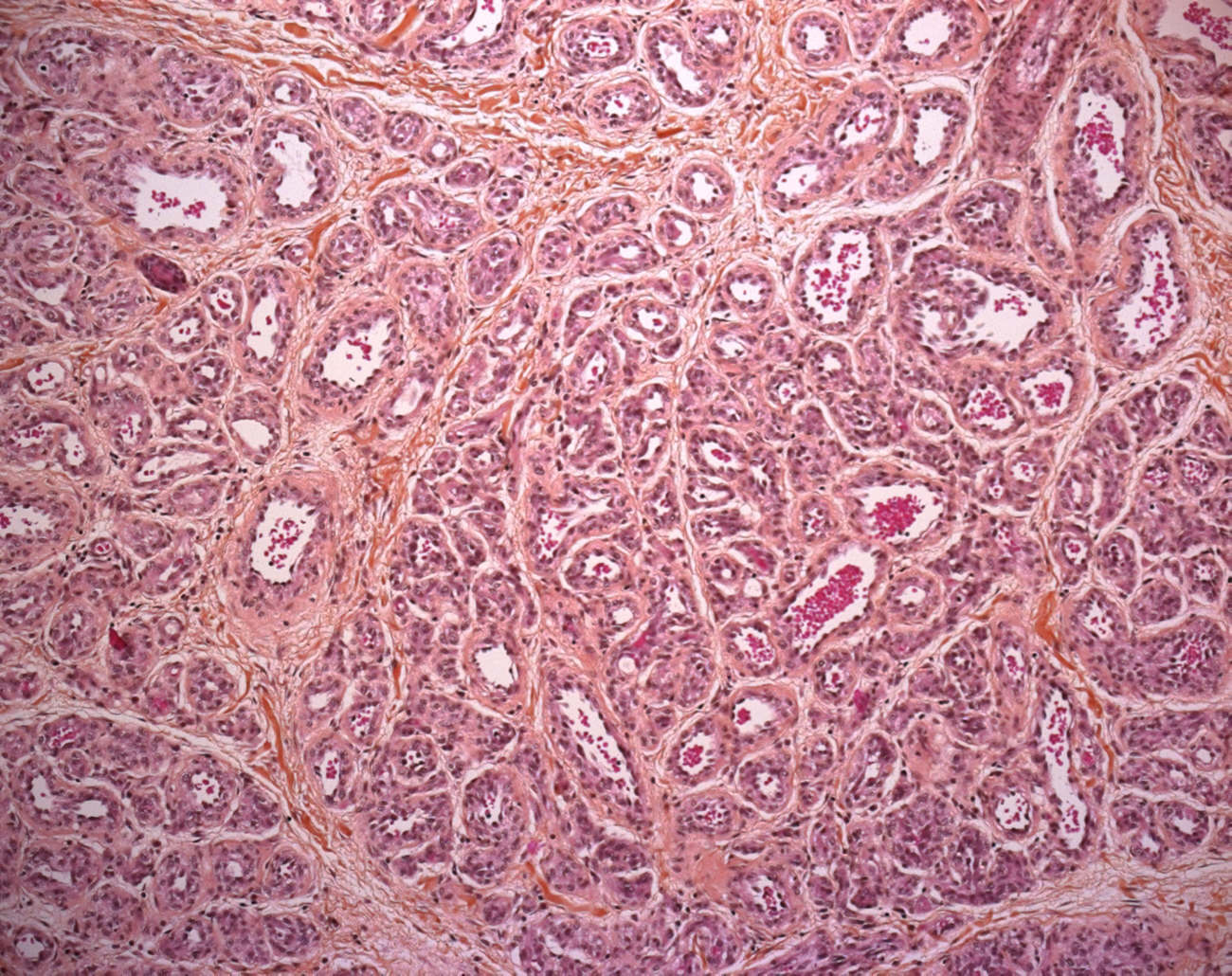
These tumors are highly cellular, involving the dermis, often with extension into the subcutis. The tumor has a lobular architecture and plump endothelial cells. The latter cells express glut-1 antigens throughout the life of this tumor.
lobular architecture
Developmental phases:
proliferative phase
involutive phase
end-stage
Localization
cutaneous infantile hemangioma
extra-cutaneous GLUT1+ infantile hemangioma
- hepatic infantile hemangioma (15509684)
- mammary infantile haemangioma (15509684)
- salivary infantile haemangioma (15509684)
- placental infantile haemangioma (15509684)
Variants
multiple infantile hemangioma (16880251)
reticular infantile hemangioma (17845155)
Associations
type 2 infantile hepatic hemangioendothelioma (16880251)
Differential diagnosis
congenital hemangiomas
vascular malformations
Immunochemsitry
WT1+
GLUT1+ (16230568)
| Tumors | GLUT1 | WT1 |
| infantile hemangioma | + | + |
| vascular malformation | - | - |
Predisposition
Beckwith-Wiedemann syndrome (15509684)
familial predisposition at locus 5q31-33
Molecular biology
monoclonality
β-Adrenergic receptor expression in vascular tumors (22743651)
Propranolol has recently emerged as an effective therapy for infantile hemangiomas causing regression.
The β-adrenergic receptor (AR) antagonist is thought to cause vasoconstriction by its effect on nitric oxide, block angiogenesis by its effect on vascular endothelial growth factor (VEGF), and induce apoptosis.
The expression of β2-AR (B2-AR) and its phosphorylated form (B2-ARP) have been identified in a case of infantile hemangioma that responded to propranolol treatment.
Although immunohistochemical expression of the receptors does not necessarily indicate that similar pathways of responsiveness to β-blockade are present, it does raises the possibility that β-blockade could potentially affect apoptosis and decrease responsiveness to VEGF.
See also
vascular tumors
vascular malformations (vascular dysplasia)
cutaneous tumors
Reviews
Vikkula M, Boon LM, Mulliken JB, Olsen BR. Molecular basis of vascular anomalies. Trends Cardiovasc Med. 1998 Oct;8(7):281-92. PMID: 14987552
References
β-Adrenergic receptor expression in vascular tumors. Chisholm KM, Chang KW, Truong MT, Kwok S, West RB, Heerema-McKenney AE. Mod Pathol. 2012 Jun 29. PMID: 22743651
Lawley LP, Cerimele F, Weiss SW, North P, Cohen C, Kozakewich HP, Mulliken JB, Arbiser JL. Expression of Wilms tumor 1 gene distinguishes vascular malformations from proliferative endothelial lesions. Arch Dermatol. 2005 Oct;141(10):1297-300. PMID: 16230568
Timar J, Meszaros L, Orosz Z, Albini A, Raso E. WT1 expression in angiogenic tumours of the skin. Histopathology. 2005 Jul;47(1):67-73. PMID: 15982325
Dadras SS, North PE, Bertoncini J, Mihm MC, Detmar M. Infantile hemangiomas are arrested in an early developmental vascular differentiation state. Mod Pathol. 2004 Sep;17(9):1068-79. PMID: 15143338

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}