Home > G. Tumoral pathology > embryonal carcinoma
embryonal carcinoma
Monday 8 November 2004
| WP |
Definition: Embryonal carcinoma is relatively common among testicular germ cell tumors, where 10% are pure embryonal carcinomas and even more have it as a component of a mixed germ cell tumor. For unknown reasons, embryonal carcinoma is rare among ovarian germ cell tumors.
Images
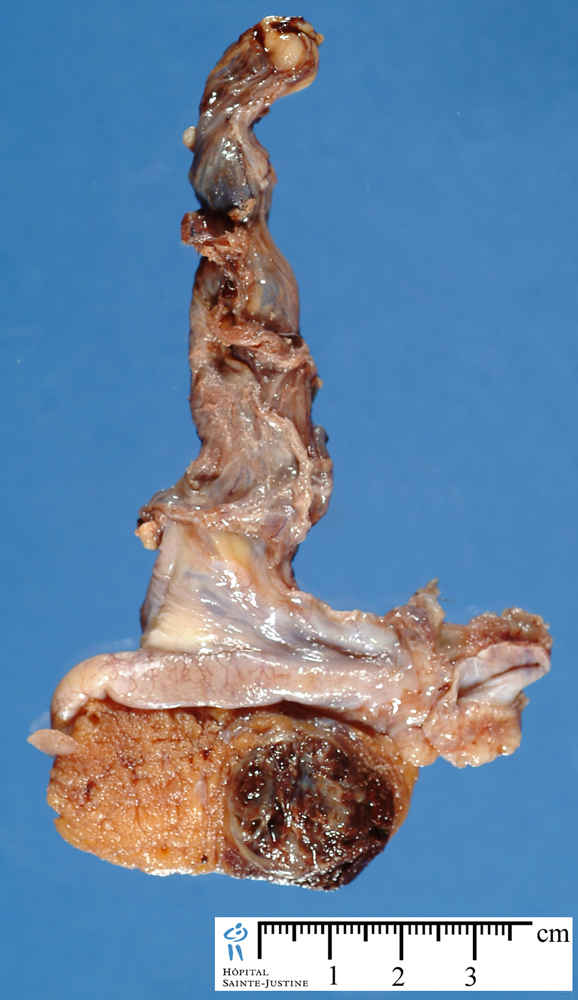
Macroscopy
Microscopy
Embryonal carcinoma is relatively common among testicular germ cell tumors, where 10% are pure embryonal carcinomas and even more have it as a component of a mixed germ cell tumor. Yet, for unknown reasons, embryonal carcinoma is rare among ovarian germ cell tumors.
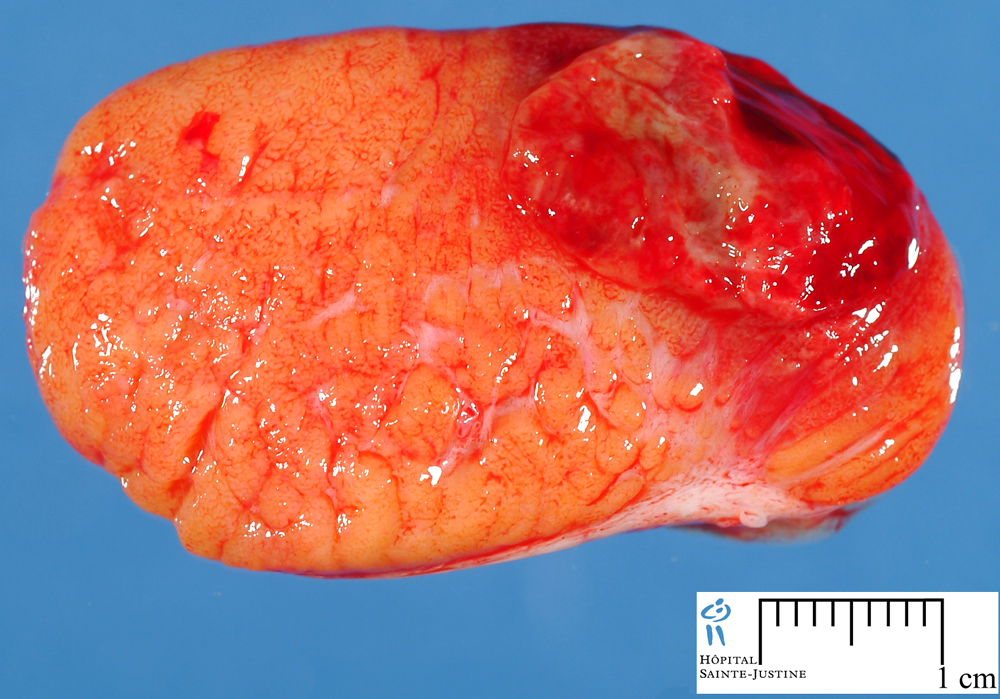
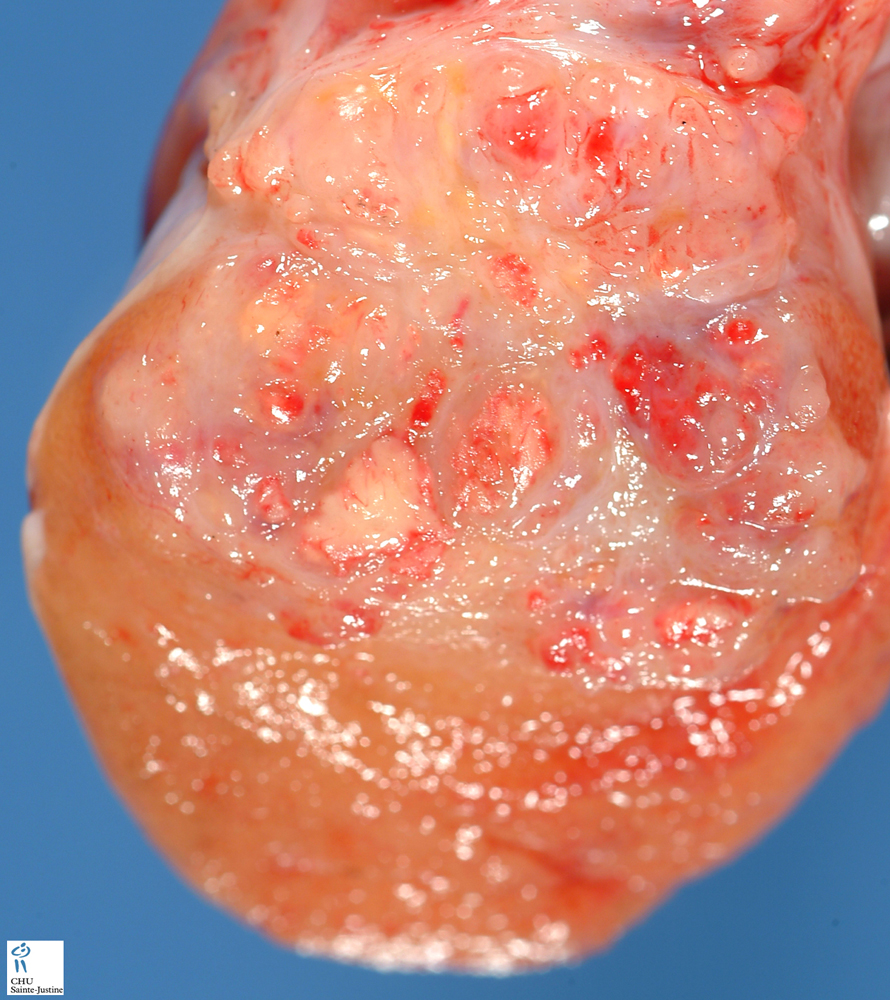
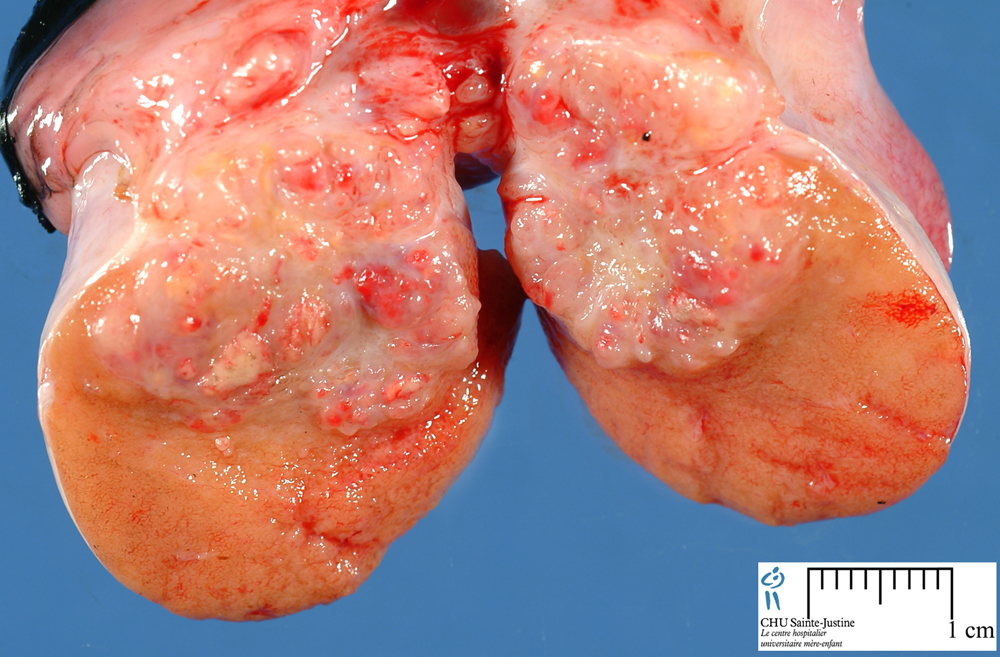
Macroscopy
The gross examination usually shows a two to three centimetre pale grey, poorly defined tumour with associated haemorrhage and necrosis.
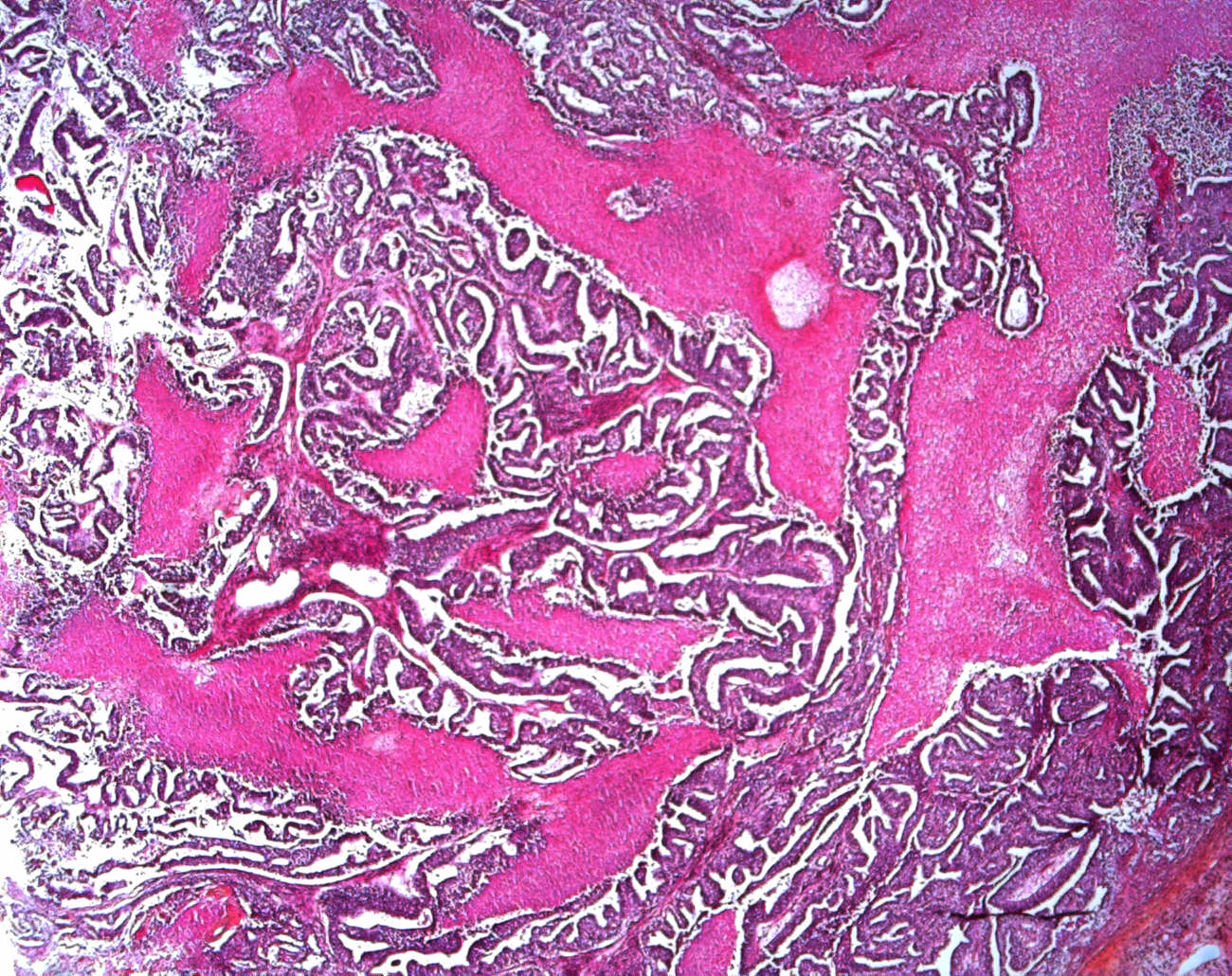
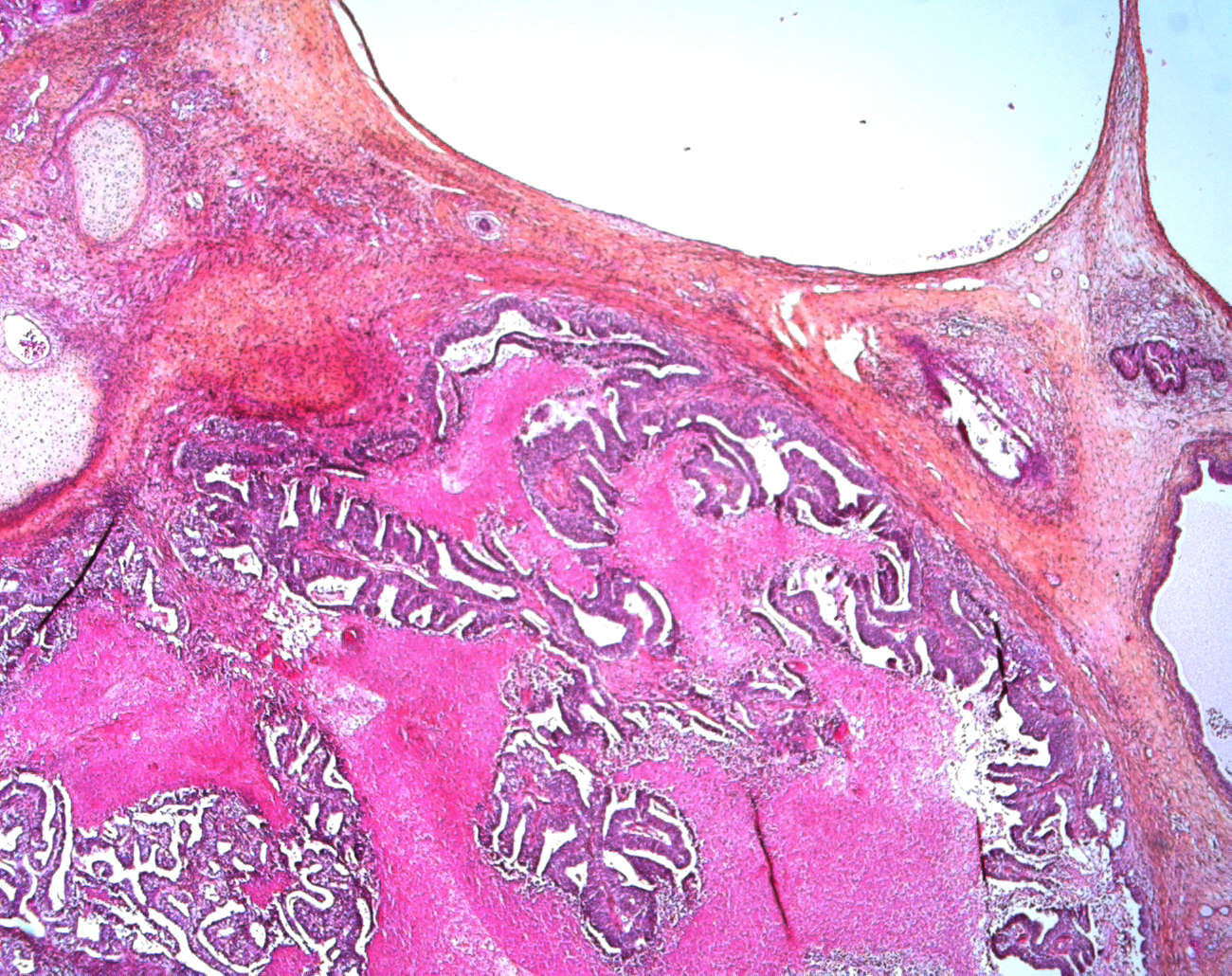
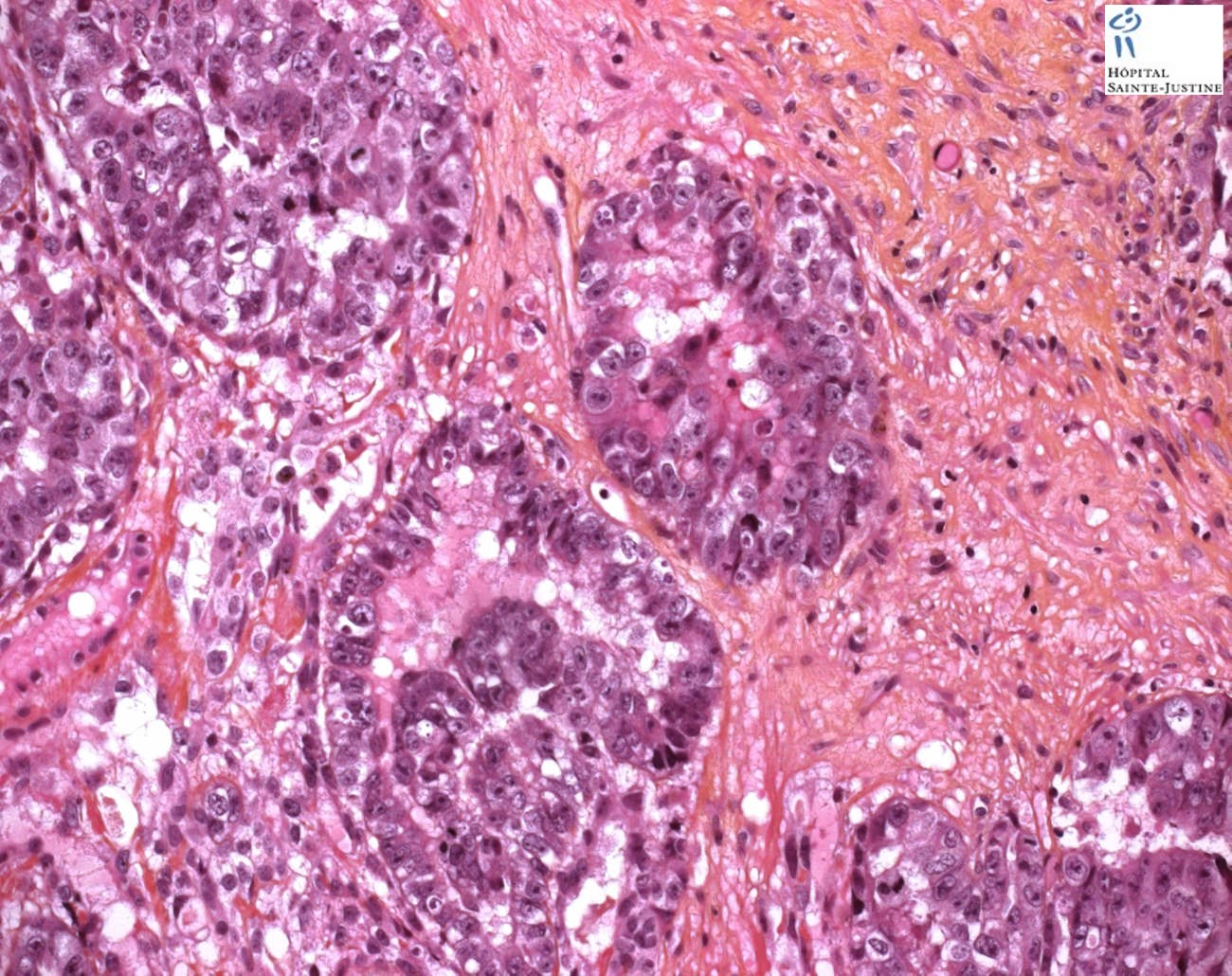
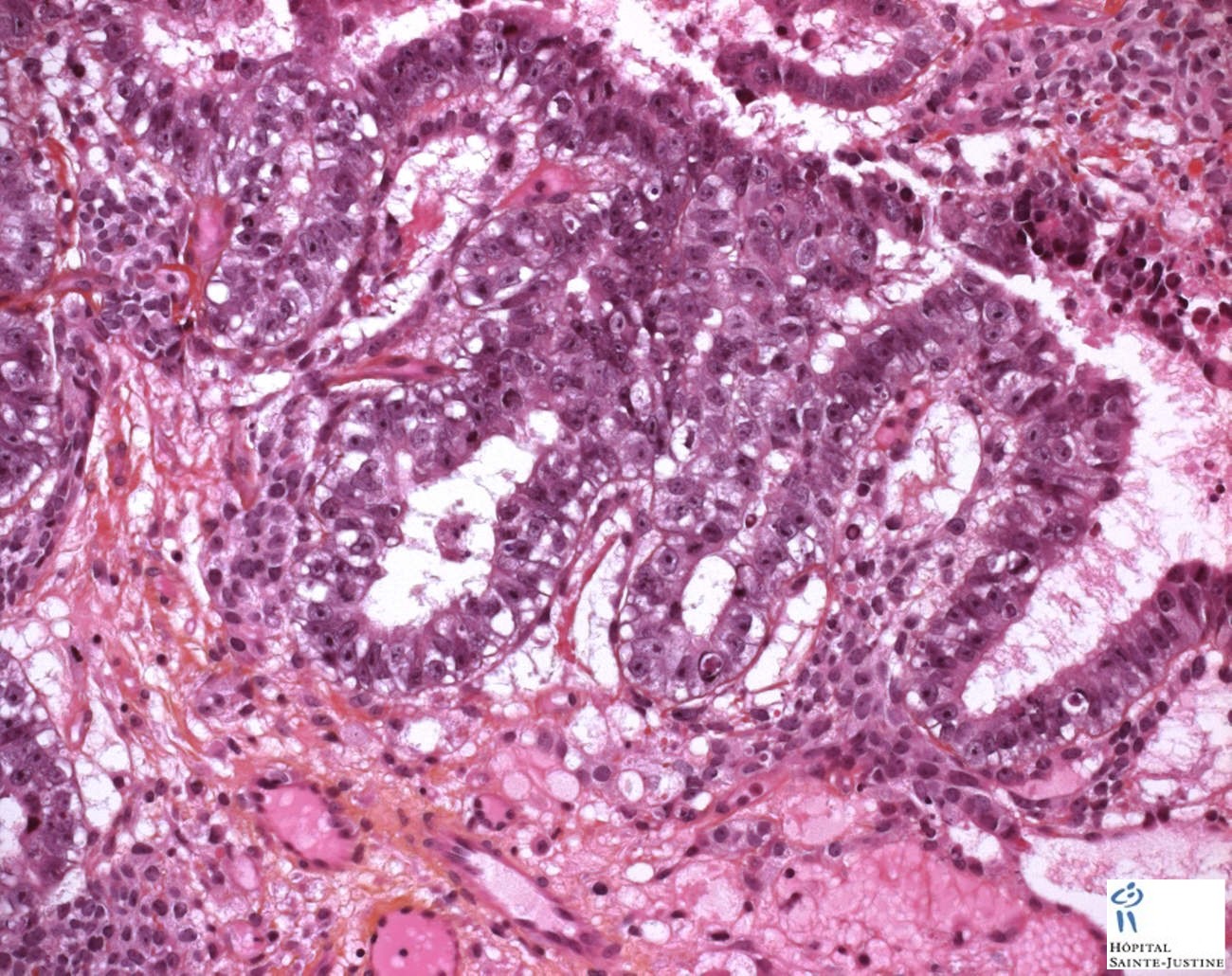
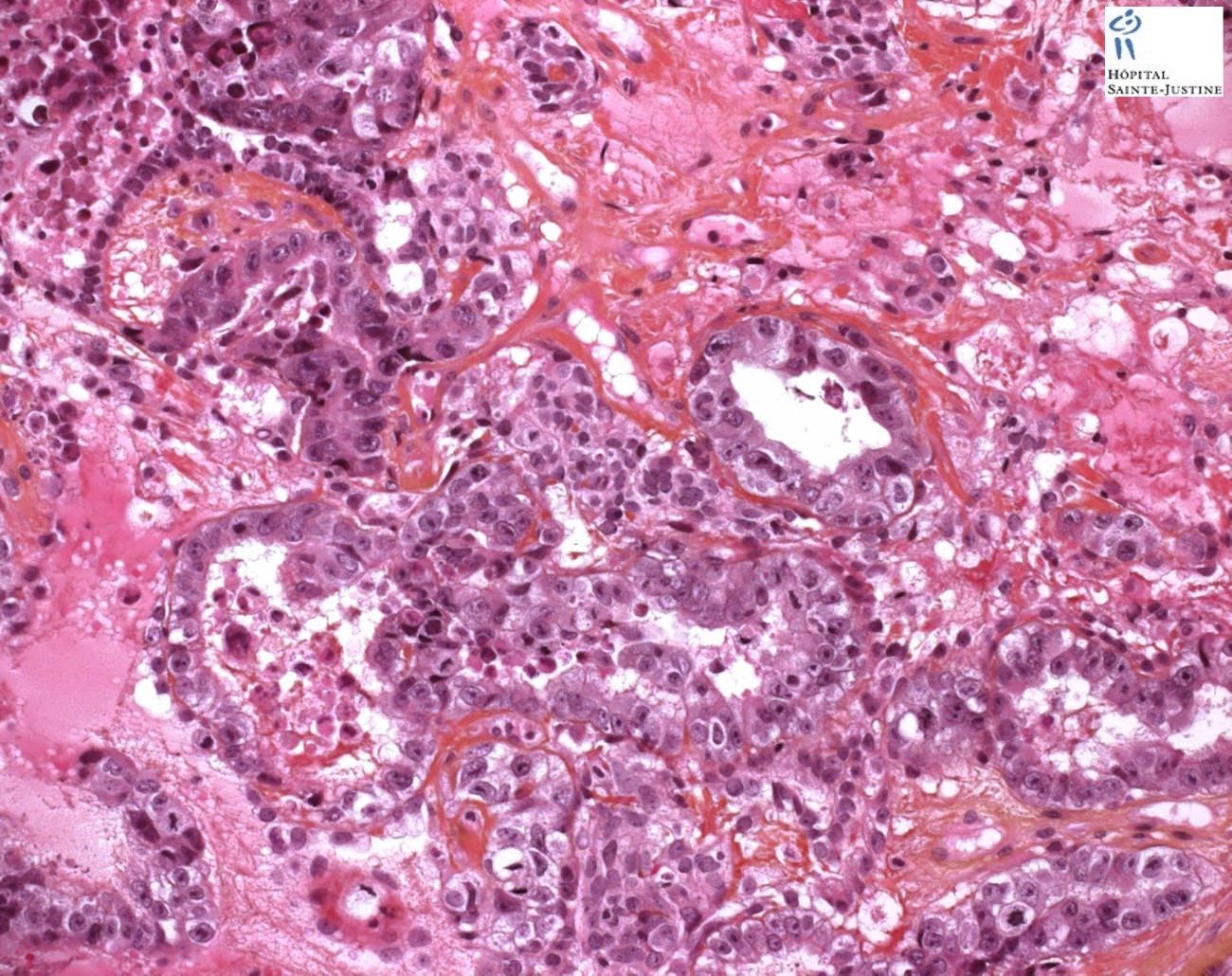
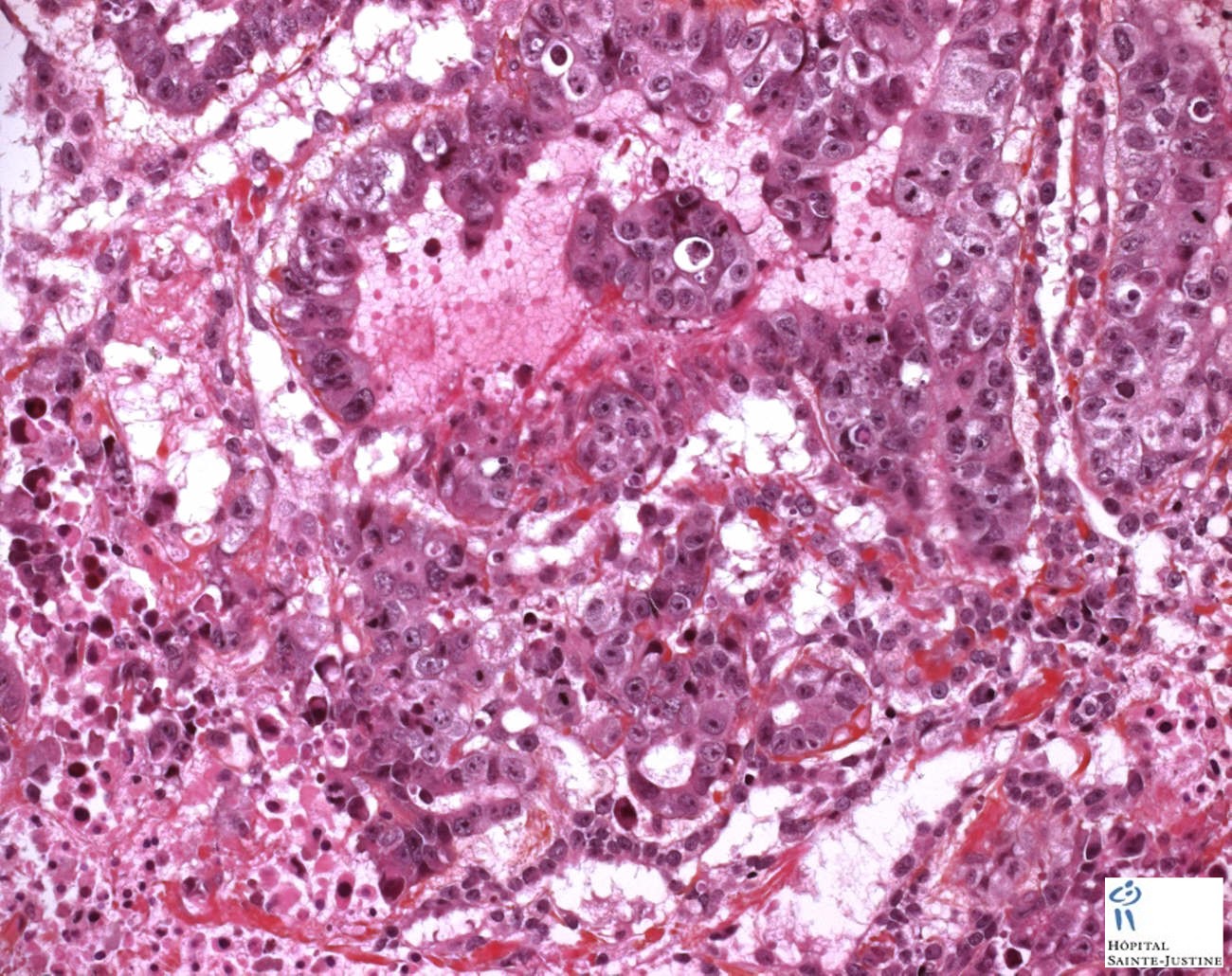
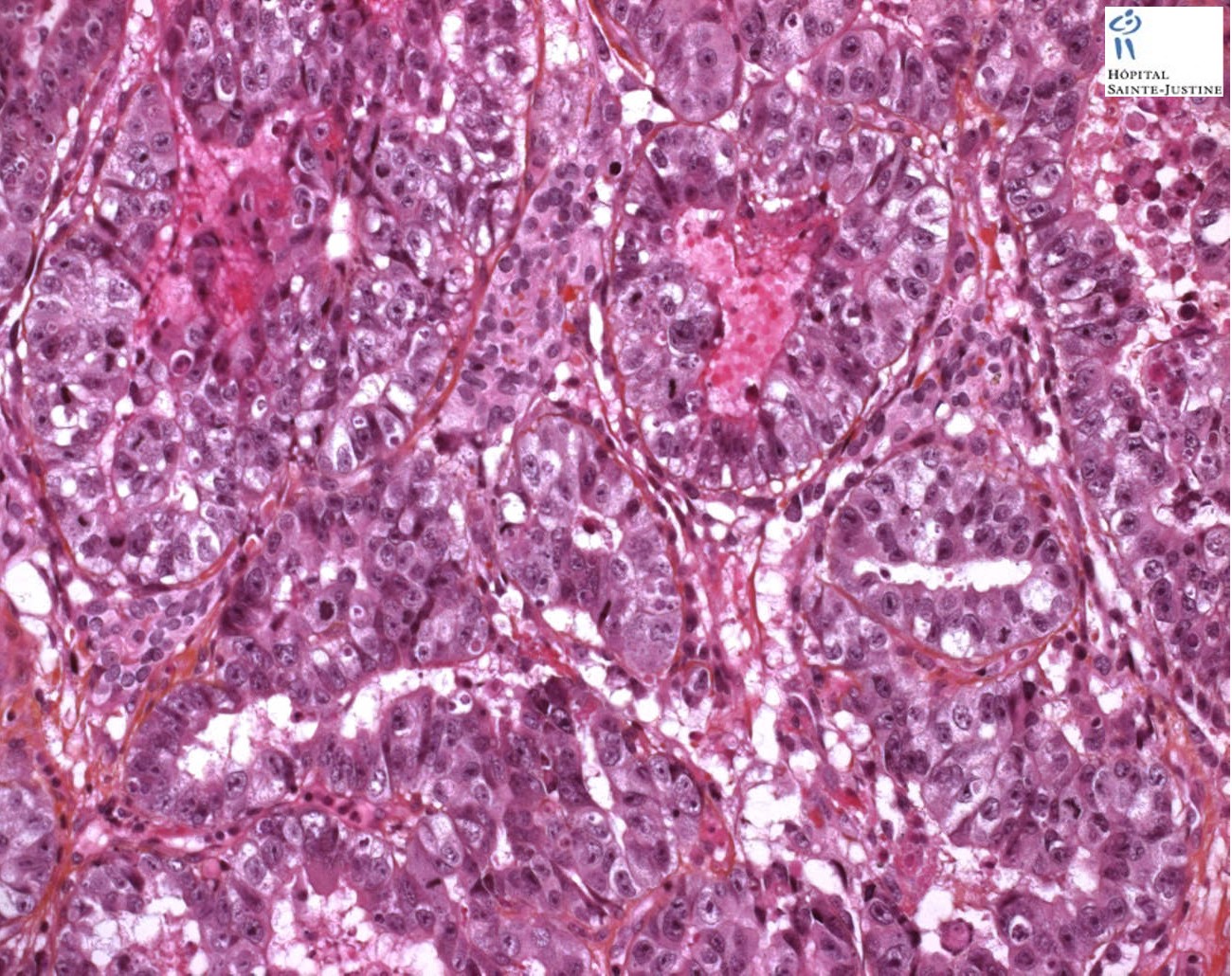
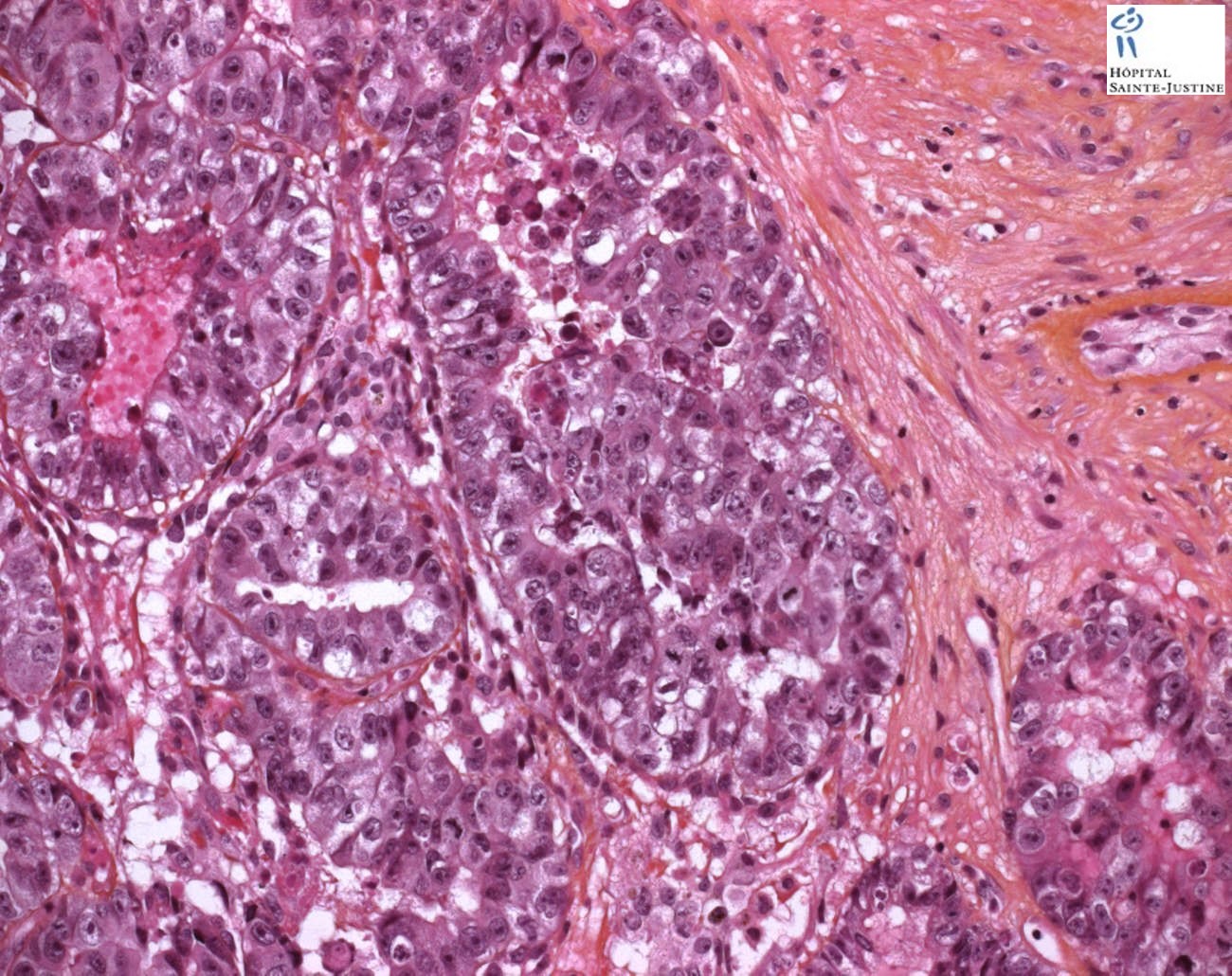
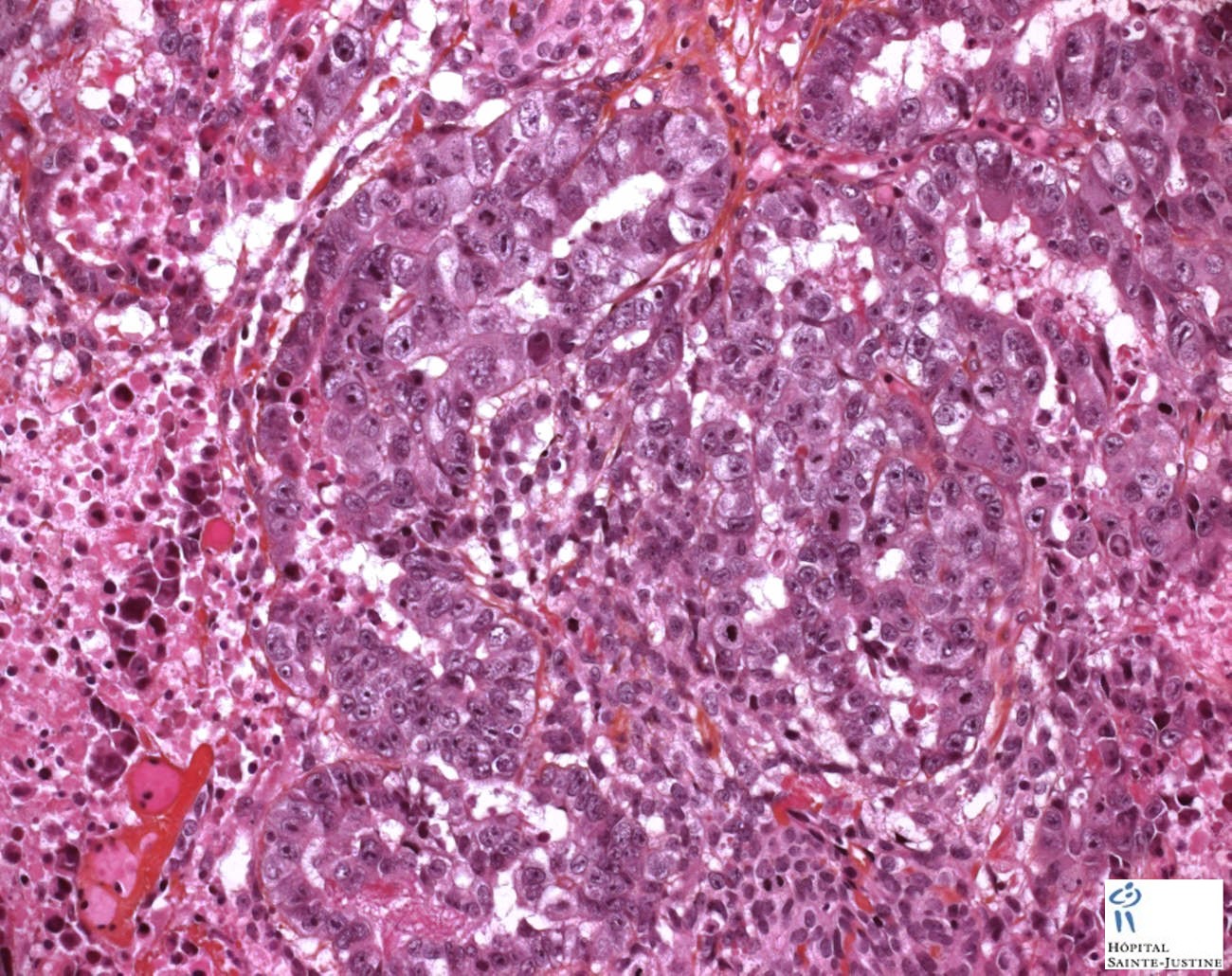
Microscopy
The microscopic features include:
indistinct cell borders,
mitoses,
variable architecture (tubulopapillary, glandular, solid),
possible embryoid bodies (ball of cells surrounded by empty space on three sides),
nuclear overlap,
necrosis.
Immunochemistry
Embryonal carcinomas are typically positive for placental alkaline phosphatase (PLAP), c-kit (CD117), keratins (8, 18, 19), and CD30.
In addition, embryonal carcinomas test positive for other markers now being used in the diagnosis, including NANOG, SOX2 (sex-determining region Y [SRY] – box 2), and OCT3/4.
Seminomas are negative for CD30 and SOX2—a fact that should help in the differential diagnosis.
AFP is only rarely positive in scattered embryonal carcinoma cells and usually distinguishes yolk sac areas.
Testicular embryonal carcinoma
In the testis, pure embryonal carcinoma is also uncommon, and accounts for approximately ten percent of testicular germ cell tumours. However, it is present as a component of almost ninety percent of mixed nonseminomatous germ cell tumours.
The average age at diagnosis is 31 years, and typically presents as a testicular lump which may be painful.
One fifth to two thirds of patients with tumours composed predominantly of embryonal carcinoma have metastases at diagnosis.
Ovarian embryonal carcinoma
In the ovary, embryonal carcinoma is quite rare, amounting to approximately three percent of ovarian germ cell tumours. The median age at diagnosis is 15 years. Symptoms and signs are varied, and may include sexual precocity and abnormal (increased, reduced or absent) uterine bleeding.
There may be elevations in serum human chorionic gonadotropin (hCG) and alpha fetoprotein (AFP) levels but it would be in association with other tumors, (e.g. yolk sac tumor,) because they themselves do not produce the serum markers.
At surgery, there is extension of the tumour beyond the ovary in forty percent of cases. They are generally large, unilateral tumours, with a median diameter of 17 centimetres. Long term survival has improved following the advent of chemotherapy.
The gross and histologic features of this tumour are similar to that seen in the testis.
Differential diagnosis
seminoma (vacuolated),
teratocarcinoma (3 differentiated germ layers),
yolk sac tumor (Schiller-Duval bodies),
Sertoli-Leydig cell tumor (strings of glands)
An important key to distinguish it from other tumors is that the embryonal carcinoma cells are "trying" to evolve into their next stage of development. So in the testicle, they are often observed as blue cells attempting to form primitive tubules.
The sheets, glands, and papillary structures composed of primitive epithelial cells with crowded, pleomorphic nuclei are usually distinctive among the germ cell tumors and pose no diagnostic problem in the gonad except for their distinction from uncommon atypical seminomas, as already discussed.
When patients, however, present with metastatic lesions without a known gonadal primary, the distinction from an undifferentiated large cell carcinoma can be problematic.
The typically younger age of the patient, however, is helpful, and a panel of immunostains that includes CD30, EMA, and OCT3/4 can confirm the diagnosis in this situation.
See also
germ cell tumors


{kind=link}
{kind=link}